

Estrogen rescues preexisting severe pulmonary hypertension in rats
- PMID: 21700911
- PMCID: PMC3208600
- DOI: 10.1164/rccm.201101-0078OC
Estrogen rescues preexisting severe pulmonary hypertension in rats
Abstract
Rationale: Pulmonary hypertension (PH) is characterized by progressive increase in pulmonary artery pressure leading to right ventricular (RV) hypertrophy, RV failure, and death. Current treatments only temporarily reduce severity of the disease, and an ideal therapy is still lacking.
Objectives: Estrogen pretreatment has been shown to attenuate development of PH. Because PH is not often diagnosed early, we examined if estrogen can rescue preexisting advanced PH.
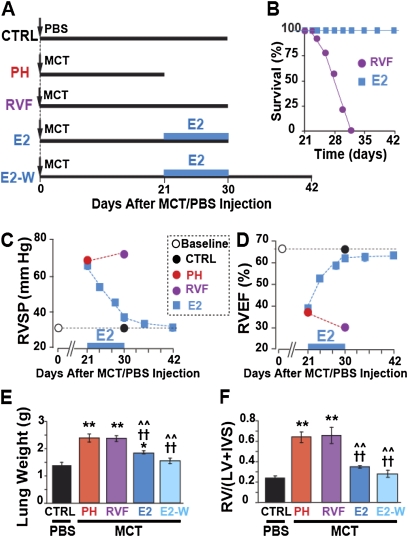
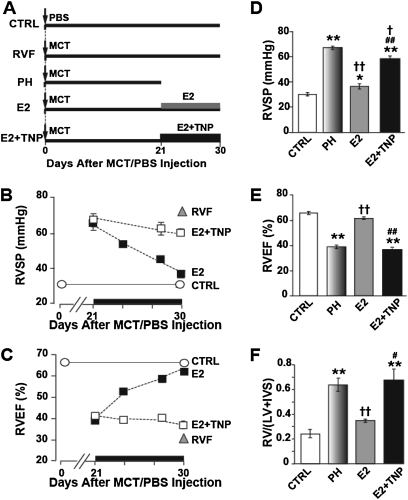
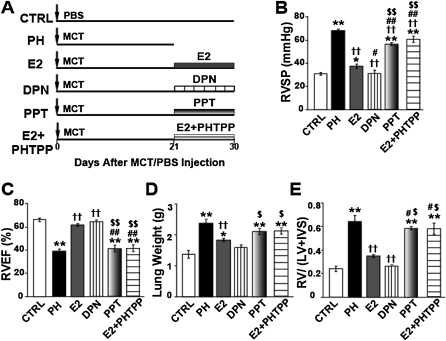
Methods: PH was induced in male rats with monocrotaline (60 mg/kg). At Day 21, rats were either treated with 17-β estradiol or estrogen (E2, 42.5 μg/kg/d), estrogen receptor-β agonist (diarylpropionitrile, 850 μg/kg/d), or estrogen receptor α-agonist (4,4',4"-[4-Propyl-(1H)-pyrazole-1,3,5-triyl] trisphenol, 850 μg/kg/d) for 10 days or left untreated to develop RV failure. Serial echocardiography, cardiac catheterization, immunohistochemistry, Western blot, and real-time polymerase chain reaction were performed.
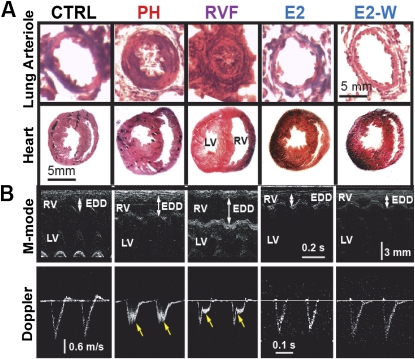
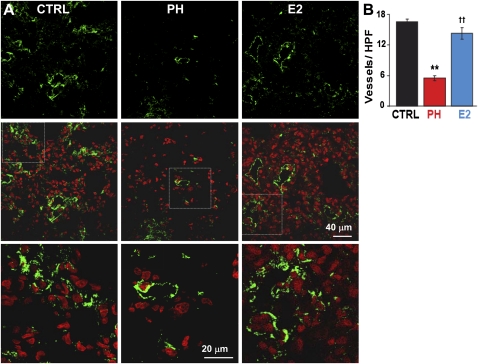
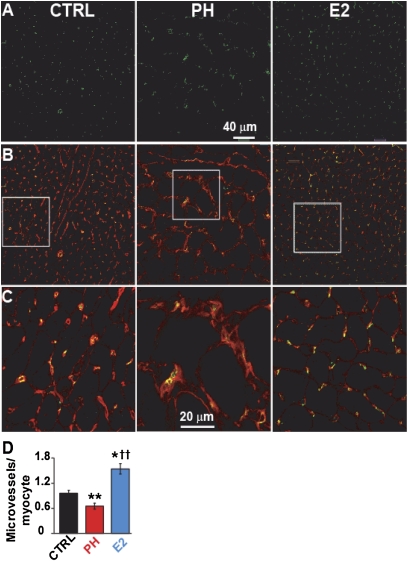
Measurements and main results: Estrogen therapy prevented progression of PH to RV failure and restored lung and RV structure and function. This restoration was maintained even after removal of estrogen at Day 30, resulting in 100% survival at Day 42. Estradiol treatment restored the loss of blood vessels in the lungs and RV. In the presence of angiogenesis inhibitor TNP-470 (30 mg/kg) or estrogen receptor-β antagonist (PHTPP, 850 μg/kg/d), estrogen failed to rescue PH. Estrogen receptor-β selective agonist was as effective as estrogen in rescuing PH.
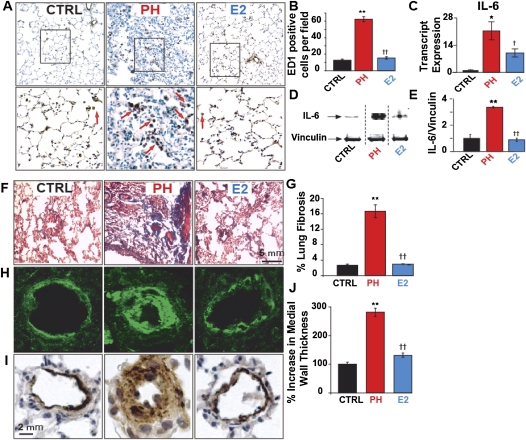
Conclusions: Estrogen rescues preexisting severe PH in rats by restoring lung and RV structure and function that are maintained even after removal of estrogen. Estrogen-induced rescue of PH is associated with stimulation of cardiopulmonary neoangiogenesis, suppression of inflammation, fibrosis, and RV hypertrophy. Furthermore, estrogen rescue is likely mediated through estrogen receptor-β.
Figures
Comment in
-
Making sense of the estrogen paradox in pulmonary arterial hypertension.Am J Respir Crit Care Med. 2011 Sep 15;184(6):629-30. doi: 10.1164/rccm.201107-1184ED. Am J Respir Crit Care Med. 2011. PMID: 21920924 No abstract available.
Similar articles
-
Reverse right ventricular structural and extracellular matrix remodeling by estrogen in severe pulmonary hypertension.J Appl Physiol (1985). 2012 Jul;113(1):149-58. doi: 10.1152/japplphysiol.01349.2011. Epub 2012 May 24. J Appl Physiol (1985). 2012. PMID: 22628376 Free PMC article.
-
Intralipid prevents and rescues fatal pulmonary arterial hypertension and right ventricular failure in rats.Hypertension. 2011 Sep;58(3):512-8. doi: 10.1161/HYPERTENSIONAHA.110.168781. Epub 2011 Jul 11. Hypertension. 2011. PMID: 21747043 Free PMC article.
-
Genistein, a soy phytoestrogen, reverses severe pulmonary hypertension and prevents right heart failure in rats.Hypertension. 2012 Aug;60(2):425-30. doi: 10.1161/HYPERTENSIONAHA.112.191445. Epub 2012 Jul 2. Hypertension. 2012. PMID: 22753213 Free PMC article.
-
Estrogen paradox in pulmonary hypertension: current controversies and future perspectives.Am J Respir Crit Care Med. 2012 Jul 15;186(2):125-31. doi: 10.1164/rccm.201201-0058PP. Epub 2012 May 3. Am J Respir Crit Care Med. 2012. PMID: 22561960 Free PMC article. Review.
-
The Role of Thyroid Disorders, Obesity, Diabetes Mellitus and Estrogen Exposure as Potential Modifiers for Pulmonary Hypertension.J Clin Med. 2022 Feb 10;11(4):921. doi: 10.3390/jcm11040921. J Clin Med. 2022. PMID: 35207198 Free PMC article. Review.
Cited by
-
Hypoxia-induced pulmonary hypertension upregulates eNOS and TGF-β contributing to sex-linked differences in BMPR2 +/R899X mutant mice.Pulm Circ. 2022 Oct 1;12(4):e12163. doi: 10.1002/pul2.12163. eCollection 2022 Oct. Pulm Circ. 2022. PMID: 36484056 Free PMC article.
-
Sex and gender in pulmonary arterial hypertension.Eur Respir Rev. 2021 Nov 8;30(162):200330. doi: 10.1183/16000617.0330-2020. Print 2021 Dec 31. Eur Respir Rev. 2021. PMID: 34750113 Free PMC article. Review.
-
Morphological and Functional Characteristics of Animal Models of Myocardial Fibrosis Induced by Pressure Overload.Int J Hypertens. 2020 Jan 31;2020:3014693. doi: 10.1155/2020/3014693. eCollection 2020. Int J Hypertens. 2020. PMID: 32099670 Free PMC article. Review.
-
Transcriptomic analysis of pulmonary artery smooth muscle cells identifies new potential therapeutic targets for idiopathic pulmonary arterial hypertension.Br J Pharmacol. 2020 Aug;177(15):3505-3518. doi: 10.1111/bph.15074. Epub 2020 May 15. Br J Pharmacol. 2020. PMID: 32337710 Free PMC article.
-
Gender, sex hormones and pulmonary hypertension.Pulm Circ. 2013 Apr;3(2):294-314. doi: 10.4103/2045-8932.114756. Pulm Circ. 2013. PMID: 24015330 Free PMC article. Review.
References
-
- Umar S, de Visser YP, Steendijk P, Schutte CI, Laghmani EH, Wagenaar GTM, Bax WH, Mantikou E, Pijnappels DA, Atsma DE, et al. Allogenic stem cell therapy improves right ventricular function by improving lung pathology in rats with pulmonary hypertension. Am J Physiol Heart Circ Physiol 2009;297:H1606–H1616 - PubMed
-
- Takemiya K, Kai H, Yasukawa H, Tahara N, Kato S, Imaizumi T. Mesenchymal stem cell-based prostacyclin synthase gene therapy for pulmonary hypertension rats. Basic Res Cardiol 2010;105:409–417 - PubMed
-
- Wang XX, Zhang FR, Shang YP, Zhu JH, Xie XD, Tao QM, Zhu JH, Chen JZ. Transplantation of autologous endothelial progenitor cells may be beneficial in patients with idiopathic pulmonary arterial hypertension: a pilot randomized controlled trial. J Am Coll Cardiol 2007;49:1566–1571 - PubMed
-
- Yen CH, Leu S, Lin YC, Kao YH, Chang LT, Chua S, Fu M, Wu CJ, Sun CK, Yip HK. Sildenafil limits monocrotaline-induced pulmonary hypertension in rats through suppression of pulmonary vascular remodeling. J Cardiovasc Pharmacol 2010;55:574–584 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
