

Prevalence of anaemia and immunological markers among ghanaian HAART-naïve HIV-patients and those on HAART
- PMID: 21572851
- PMCID: PMC3092327
Prevalence of anaemia and immunological markers among ghanaian HAART-naïve HIV-patients and those on HAART
Abstract
Background: Highly active antiretroviral therapy (HAART) for people living with HIV/AIDS (PLWHA) has been generally accepted as the gold standard for the management of HIV patients but conflicting reports about the ability of HAART to improve upon the quality of life of HIV patients has cast doubts over the efficacy and the need for therapy.
Objective: This study was conducted to assess the efficacy and ability of HAART to resolve immunological and haematological abnormalities in HIV infected patients, existent sex variations in immunological and haematological parameters and CD4 predictive ability of the study parameters.
Methods: A total of 442 PLWHA consisting of 166 patients on HAART (28 males and 138 females) and 276 HAART-naïve patients (76 males and 200 females) were recruited for this study. Complete haemogram, immunological analysis (CD4 & CD3) and weight were measured for all the patients.
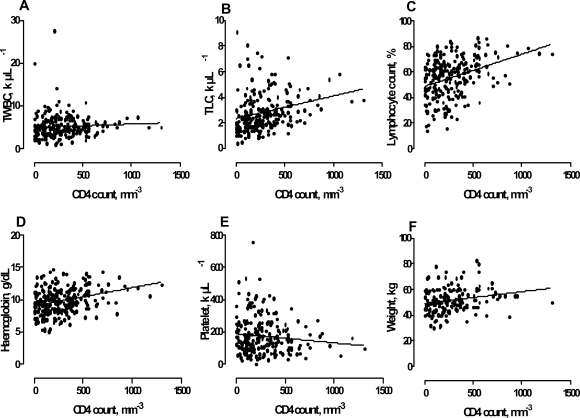
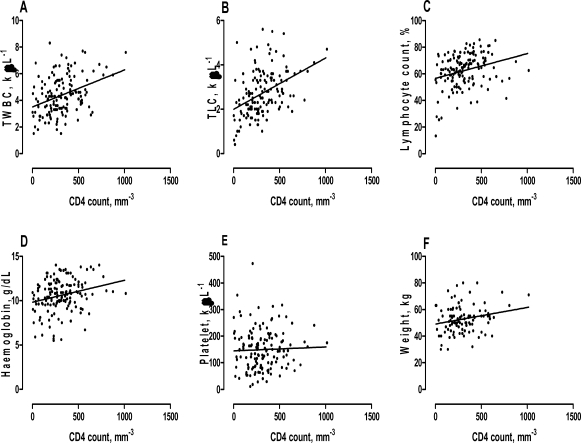
Results: HAART patients were older and heavier than their naïve counterparts. The incidence of anaemia (Hb less or equal to 10.5 (63%) and PCV < 30% (37.6%)) and lymphopoenia (16.7%) in HAART-naïve patients was significantly higher compared to their counterparts on HAART (46%, 15.2% and 5.3%) respectively. 70% of HAART-naïve females had anaemia in comparison to 44% in HAART-naïve males (P = 0.0001). The likelihood of developing microcytic hypochromic anaemia in HAART-naïve patients was 5 times more compared to those on HAART (P = 0.0002). Total lymphocyte count, haemoglobin, lymphocyte count and weight were significant predictors of CD4 counts and TLC values between 1.0 - 2.0 k µL(-1) was a significant predictor of CD4 <200 cells mm(-3).
Conclusion: HAART has the capability of reducing the incidence of anaemia and lymphopoenia which are associated with disease progression and death in HIV infected patients. Total lymphocyte count, haemoglobin and weight could also serve as useful predictive tools in the management and monitoring of HIV infected patients in resource limited settings.
Keywords: Antiretroviral; CD4; Lymphocyte; TLC; WHO/ACTG.
Figures
Similar articles
-
Prevalence of anaemia among HIV-infected patients in Benin City, Nigeria.Tanzan J Health Res. 2009 Jan;11(1):1-4. doi: 10.4314/thrb.v11i1.43242. Tanzan J Health Res. 2009. PMID: 19445097
-
Prevalence of Anemia and Immunological Markers in HIV-Infected Patients on Highly Active Antiretroviral Therapy in Northeastern Nigeria.Infect Dis (Auckl). 2013 Mar 20;6:25-33. doi: 10.4137/IDRT.S10477. eCollection 2013. Infect Dis (Auckl). 2013. PMID: 24847174 Free PMC article.
-
Intestinal parasitosis in relation to CD4+T cells levels and anemia among HAART initiated and HAART naive pediatric HIV patients in a Model ART center in Addis Ababa, Ethiopia.PLoS One. 2015 Feb 6;10(2):e0117715. doi: 10.1371/journal.pone.0117715. eCollection 2015. PLoS One. 2015. PMID: 25658626 Free PMC article.
-
Study of the impact of HIV genotypic drug resistance testing on therapy efficacy.Verh K Acad Geneeskd Belg. 2001;63(5):447-73. Verh K Acad Geneeskd Belg. 2001. PMID: 11813503 Review.
-
Thymic function in HIV-infection.Dan Med J. 2013 Apr;60(4):B4622. Dan Med J. 2013. PMID: 23651726 Review.
Cited by
-
Prevalence and correlates of anemia among HIV infected patients on highly active anti-retroviral therapy at Zewditu Memorial Hospital, Ethiopia.BMC Hematol. 2015 Apr 30;15:6. doi: 10.1186/s12878-015-0024-6. eCollection 2015. BMC Hematol. 2015. PMID: 26045966 Free PMC article.
-
Anaemia and zidovudine-containing antiretroviral therapy in paediatric antiretroviral programmes in the IeDEA Paediatric West African Database to evaluate AIDS.J Int AIDS Soc. 2013 Sep 17;16(1):18024. doi: 10.7448/IAS.16.1.18024. J Int AIDS Soc. 2013. PMID: 24047928 Free PMC article.
-
Immuno-haematologic and virologic responses and predictors of virologic failure in HIV-1 infected adults on first-line antiretroviral therapy in Cameroon.Infect Dis Poverty. 2014 Jan 30;3(1):5. doi: 10.1186/2049-9957-3-5. Infect Dis Poverty. 2014. PMID: 24479873 Free PMC article.
-
Immuno-Haematological Abnormalities of HIV-Infected Patients Before and After Initiation of Highly Active Antiretroviral Therapy in the Antiretroviral Therapy Clinics of Six Health Facilities at Dessie Town, Northeast Ethiopia.J Blood Med. 2022 May 11;13:243-253. doi: 10.2147/JBM.S364700. eCollection 2022. J Blood Med. 2022. PMID: 35592587 Free PMC article.
-
A Case-Control Study of the MTHFR C665T Gene Polymorphism on Macrocytic Anemia Among HIV-Infected Patients Receiving Zidovudine.J Multidiscip Healthc. 2022 Jul 29;15:1633-1641. doi: 10.2147/JMDH.S370536. eCollection 2022. J Multidiscip Healthc. 2022. PMID: 35937309 Free PMC article.
References
-
- Okolie MN, Eghafona NO, Omoregie R. Anti-human immunodeficiency virus agents. Journal of Medical Laboratory Science. 2003;12:1–14.
-
- Voth R, Rossol S, Graff E, Laubenstein HP, Schroder HC, Muller WE, Meyer zum Buschenfelde KH, Hess G. Natural killer cell activity as a prognostic parameter in the progression to AIDS. J Infect Dis. 1988;157(4):851–852. - PubMed
-
- Tersmette M, Schuitemaker H. Virulent HIV strains? AIDS. 1993;7(8):1123–1125. - PubMed
-
- Coyle TE. Hematologic complications of human immunodeficiency virus infection and the acquired immunodeficiency syndrome. Med Clin North Am. 1997;81(2):449–470. - PubMed
-
- Salond E. Haematologic complications of HIV infection. AIDS Rev. 2005;7:187–196. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous