

High-dose zidovudine plus valganciclovir for Kaposi sarcoma herpesvirus-associated multicentric Castleman disease: a pilot study of virus-activated cytotoxic therapy
- PMID: 21487108
- PMCID: PMC3143547
- DOI: 10.1182/blood-2010-11-317610
High-dose zidovudine plus valganciclovir for Kaposi sarcoma herpesvirus-associated multicentric Castleman disease: a pilot study of virus-activated cytotoxic therapy
Abstract
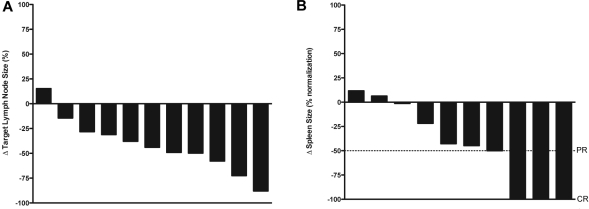
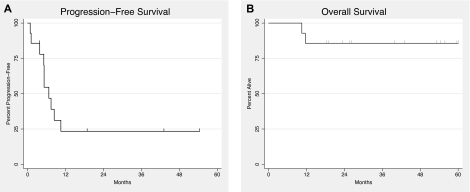
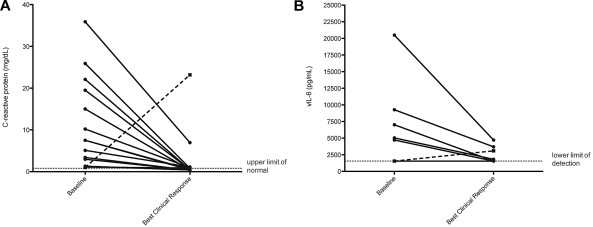
Kaposi sarcoma herpesvirus (KSHV)-associated multicentric Castleman disease (MCD) is a lymphoproliferative disorder most commonly observed in HIV-infected patients. It is characterized by KSHV-infected plasmablasts that frequently express lytic genes. Patients manifest inflammatory symptoms attributed to overproduction of KSHV viral IL-6, human IL-6, and human IL-6. There is no standard therapy and no established response criteria. We investigated an approach targeting 2 KSHV lytic genes, ORF36 and ORF21, the protein of which, respectively, phosphorylate ganciclovir and zidovudine to toxic moieties. In a pilot study, 14 HIV-infected patients with symptomatic KSHV-MCD received high-dose zidovudine (600 mg orally every 6 hours) and the oral prodrug, valganciclovir (900 mg orally every 12 hours). Responses were evaluated using new response criteria. A total of 86% of patients attained major clinical responses and 50% attained major biochemical responses. Median progression-free survival was 6 months. With 43 months of median follow-up, overall survival was 86% at 12 months and beyond. At the time of best response, the patients showed significant improvements in C-reactive protein, albumin, platelets, human IL-6, IL-10, and KSHV viral load. The most common toxicities were hematologic. These observations provide evidence that therapy designed to target cells with lytic KSHV replication has activity in KSHV-MCD. This trial was registered at www.clinicaltrials.gov as #NCT00099073.
Figures
Comment in
-
KSHV: forgotten but not gone.Blood. 2011 Jun 30;117(26):6973-4. doi: 10.1182/blood-2011-05-350306. Blood. 2011. PMID: 21719604 No abstract available.
Similar articles
-
Rituximab plus liposomal doxorubicin in HIV-infected patients with KSHV-associated multicentric Castleman disease.Blood. 2014 Dec 4;124(24):3544-52. doi: 10.1182/blood-2014-07-586800. Epub 2014 Oct 20. Blood. 2014. PMID: 25331113 Free PMC article. Clinical Trial.
-
Induction of Kaposi's Sarcoma-Associated Herpesvirus-Encoded Thymidine Kinase (ORF21) by X-Box Binding Protein 1.J Virol. 2020 Feb 14;94(5):e01555-19. doi: 10.1128/JVI.01555-19. Print 2020 Feb 14. J Virol. 2020. PMID: 31801863 Free PMC article.
-
Recent advances in Kaposi sarcoma herpesvirus-associated multicentric Castleman disease.Curr Opin Oncol. 2012 Sep;24(5):495-505. doi: 10.1097/CCO.0b013e328355e0f3. Curr Opin Oncol. 2012. PMID: 22729151 Free PMC article. Review.
-
Treatment of Kaposi Sarcoma Herpesvirus-Associated Multicentric Castleman Disease.Hematol Oncol Clin North Am. 2018 Feb;32(1):75-88. doi: 10.1016/j.hoc.2017.09.007. Hematol Oncol Clin North Am. 2018. PMID: 29157621 Free PMC article. Review.
-
Tocilizumab in patients with symptomatic Kaposi sarcoma herpesvirus-associated multicentric Castleman disease.Blood. 2020 Jun 18;135(25):2316-2319. doi: 10.1182/blood.2019004602. Blood. 2020. PMID: 32276276 Free PMC article. No abstract available.
Cited by
-
18F-fluorodeoxyglucose Positron Emission Tomography in Kaposi Sarcoma Herpesvirus-Associated Multicentric Castleman Disease: Correlation With Activity, Severity, Inflammatory and Virologic Parameters.J Infect Dis. 2015 Oct 15;212(8):1250-60. doi: 10.1093/infdis/jiv204. Epub 2015 Mar 31. J Infect Dis. 2015. PMID: 25828248 Free PMC article.
-
Characteristics and outcomes of KSHV-associated multicentric Castleman disease with or without other KSHV diseases.Blood Adv. 2021 Mar 23;5(6):1660-1670. doi: 10.1182/bloodadvances.2020004058. Blood Adv. 2021. PMID: 33720337 Free PMC article.
-
Clinical Manifestations of Kaposi Sarcoma Herpesvirus Lytic Activation: Multicentric Castleman Disease (KSHV-MCD) and the KSHV Inflammatory Cytokine Syndrome.Front Microbiol. 2012 Mar 2;3:73. doi: 10.3389/fmicb.2012.00073. eCollection 2012. Front Microbiol. 2012. PMID: 22403576 Free PMC article.
-
Viral profiling identifies multiple subtypes of Kaposi's sarcoma.mBio. 2014 Sep 23;5(5):e01633-14. doi: 10.1128/mBio.01633-14. mBio. 2014. PMID: 25249280 Free PMC article.
-
High Seroprevalence of Kaposi Sarcoma-Associated Herpesvirus in Men Who Have Sex With Men With HIV in the Southern United States.Open Forum Infect Dis. 2023 Mar 24;10(4):ofad160. doi: 10.1093/ofid/ofad160. eCollection 2023 Apr. Open Forum Infect Dis. 2023. PMID: 37096147 Free PMC article.
References
-
- Oksenhendler E, Duarte M, Soulier J, et al. Multicentric Castleman's disease in HIV infection: a clinical and pathological study of 20 patients. AIDS. 1996;10(1):61–67. - PubMed
-
- Waterston A, Bower M. Fifty years of multicentric Castleman's disease. Acta Oncol. 2004;43(8):698–704. - PubMed
-
- Chang Y, Cesarman E, Pessin MS, et al. Identification of herpesvirus-like DNA sequences in AIDS-associated Kaposi's sarcoma. Science. 1994;266(5192):1865–1869. - PubMed
-
- Soulier J, Grollet L, Oksenhendler E, et al. Kaposi's sarcoma-associated herpesvirus-like DNA sequences in multicentric Castleman's disease. Blood. 1995;86(4):1276–1280. - PubMed
-
- Teruya-Feldstein J, Zauber P, Setsuda JE, et al. Expression of human herpesvirus-8 oncogene and cytokine homologues in an HIV-seronegative patient with multicentric Castleman's disease and primary effusion lymphoma. Lab Invest. 1998;78(12):1637–1642. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
