

Association of glycemic variability and the presence and severity of coronary artery disease in patients with type 2 diabetes
- PMID: 21349201
- PMCID: PMC3056765
- DOI: 10.1186/1475-2840-10-19
Association of glycemic variability and the presence and severity of coronary artery disease in patients with type 2 diabetes
Abstract
Background: Glucose variability is one of components of the dysglycemia in diabetes and may play an important role in development of diabetic vascular complications. The objective of this study was to assess the relationship between glycemic variability determined by a continuous glucose monitoring (CGM) system and the presence and severity of coronary artery disease (CAD) in patients with type 2 diabetes mellitus (T2DM).
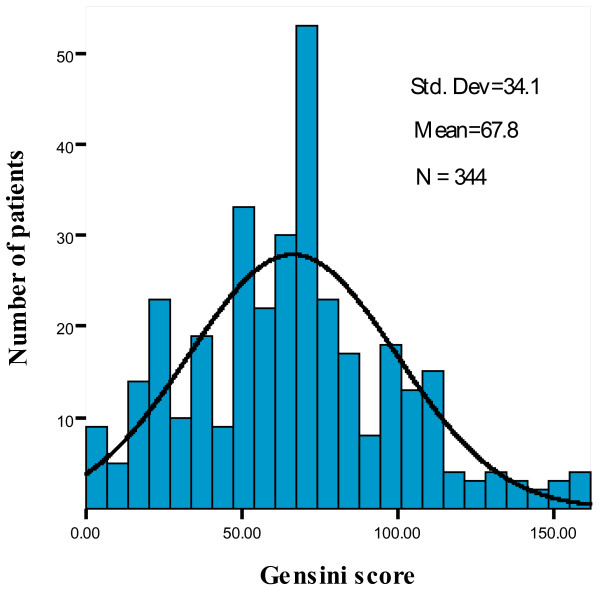
Methods: In 344 T2DM patients with chest pain, coronary angiography revealed CAD (coronary stenosis ≥ 50% luminal diameter narrowing) in 252 patients and 92 patients without CAD. Gensini score was used to assess the severity of CAD. All participants' CGM parameters and biochemical characteristics were measured at baseline.
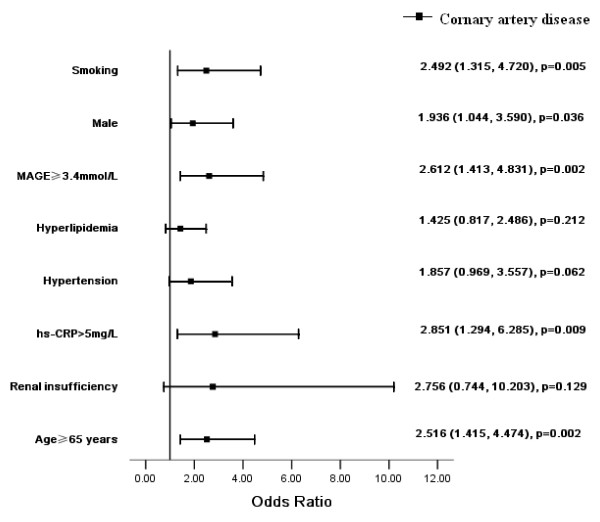
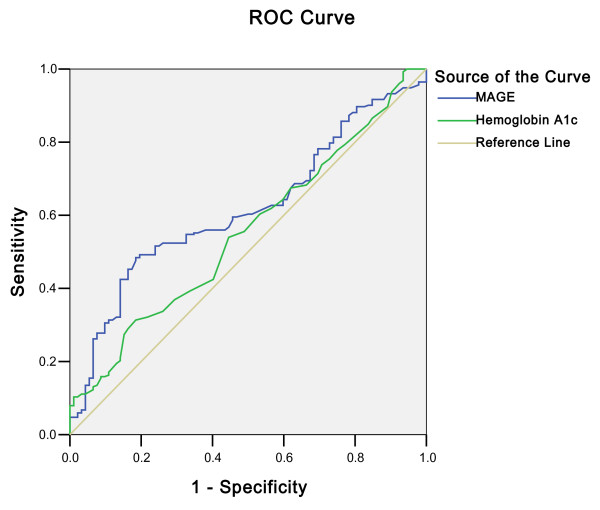
Results: Diabetic patients with CAD were older, and more were male and cigarette smokers compared with the controls. Levels of the mean amplitude of glycemic excursions (MAGE) (3.7 ± 1.4 mmol/L vs. 3.2 ± 1.2 mmol/L, p < 0.001), postprandial glucose excursion (PPGE) (3.9 ± 1.6 mmol/L vs. 3.6 ± 1.4 mmol/L, p = 0.036), serum high-sensitive C-reactive protein (hs-CRP) (10.7 ± 12.4 mg/L vs. 5.8 ± 6.7 mg/L, p < 0.001) and creatinine (Cr) (87 ± 23 mmol/L vs. 77 ± 14 mmol/L, p < 0.001) were significantly higher in patients with CAD than in patients without CAD. Gensini score closely correlated with age, MAGE, PPGE, hemoglobin A1c (HbA1c), hs-CRP and total cholesterol (TC). Multivariate analysis indicated that age (p < 0.001), MAGE (p < 0.001), serum levels of HbA1c (p = 0.022) and hs-CRP (p = 0.005) were independent determinants for Gensini score. Logistic regression analysis revealed that MAGE ≥ 3.4 mmol/L was an independent predictor for CAD. The area under the receiver-operating characteristic curve for MAGE (0.618, p = 0.001) was superior to that for HbA1c (0.554, p = 0.129).
Conclusions: The intraday glycemic variability is associated with the presence and severity of CAD in patients with T2DM. Effects of glycemic excursions on vascular complications should not be neglected in diabetes.
Figures

Similar articles
-
Comparison of glycemic variability and glycated hemoglobin as risk factors of coronary artery disease in patients with undiagnosed diabetes.Chin Med J (Engl). 2012 Jan;125(1):38-43. Chin Med J (Engl). 2012. PMID: 22340463
-
Impact of glycemic control on the association of endothelial dysfunction and coronary artery disease in patients with type 2 diabetes mellitus.Cardiovasc Diabetol. 2021 Mar 13;20(1):64. doi: 10.1186/s12933-021-01257-y. Cardiovasc Diabetol. 2021. PMID: 33714276 Free PMC article.
-
Increased serum glycated albumin level is associated with the presence and severity of coronary artery disease in type 2 diabetic patients.Circ J. 2007 Jul;71(7):1067-73. doi: 10.1253/circj.71.1067. Circ J. 2007. PMID: 17587712
-
"Mild dysglycemia" in type 2 diabetes: to be neglected or not?J Diabetes Complications. 2015 Apr;29(3):451-8. doi: 10.1016/j.jdiacomp.2014.12.004. Epub 2014 Dec 12. J Diabetes Complications. 2015. PMID: 25572605 Review.
-
Glycemic variability in the development of cardiovascular complications in diabetes.Diabetes Metab Res Rev. 2018 Nov;34(8):e3047. doi: 10.1002/dmrr.3047. Epub 2018 Aug 9. Diabetes Metab Res Rev. 2018. PMID: 30028067 Review.
Cited by
-
Unique and Varied Contributions of Traditional CVD Risk Factors: A Systematic Literature Review of CAD Risk Factors in China.Clin Med Insights Cardiol. 2013 Apr 4;7:59-86. doi: 10.4137/CMC.S10225. Print 2013. Clin Med Insights Cardiol. 2013. PMID: 23645989 Free PMC article.
-
Utility of different glycemic control metrics for optimizing management of diabetes.World J Diabetes. 2015 Feb 15;6(1):17-29. doi: 10.4239/wjd.v6.i1.17. World J Diabetes. 2015. PMID: 25685275 Free PMC article. Review.
-
Effects of glucose load and nateglinide intervention on endothelial function and oxidative stress.J Diabetes Res. 2013;2013:849295. doi: 10.1155/2013/849295. Epub 2013 Apr 7. J Diabetes Res. 2013. PMID: 23691521 Free PMC article.
-
Associations of continuous glucose monitoring-assessed glucose variability with intima-media thickness and ultrasonic tissue characteristics of the carotid arteries: a cross-sectional analysis in patients with type 2 diabetes.Cardiovasc Diabetol. 2021 May 4;20(1):95. doi: 10.1186/s12933-021-01288-5. Cardiovasc Diabetol. 2021. PMID: 33947398 Free PMC article.
-
A Randomized Pilot Study of the Effect of Trelagliptin and Alogliptin on Glycemic Variability in Patients with Type 2 Diabetes.Adv Ther. 2019 Nov;36(11):3096-3109. doi: 10.1007/s12325-019-01097-z. Epub 2019 Sep 27. Adv Ther. 2019. PMID: 31562608 Free PMC article. Clinical Trial.
References
-
- Buse JB, Ginsberg HN, Bakris GL, Clark NG, Costa F, Eckel R, Fonseca V, Gerstein HC, Grundy S, Nesto RW, Pignone MP, Plutzky J, Porte D, Redberg R, Stitzel KF, Stone NJ. American Heart Association; American Diabetes Association. Primary prevention of cardiovascular diseases in people with diabetes mellitus: a scientific statement from the American Heart Association and the American Diabetes Association. Circulation. 2007;115(1):114–126. doi: 10.1161/CIRCULATIONAHA.106.179294. - DOI - PubMed
-
- Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, Hadden D, Turner RC, Holman RR. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–412. doi: 10.1136/bmj.321.7258.405. - DOI - PMC - PubMed
-
- Sacks DB, Bruns DE, Goldstein DE, Maclaren NK, McDonald JM, Parrott M. Guidelines and recommendations for laboratory analysis in the diagnosis and management of diabetes mellitus. Clin Chem. 2002;48(3):436–472. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
