

High-end arteriolar resistance limits uterine artery blood flow and restricts fetal growth in preeclampsia and gestational hypertension at high altitude
- PMID: 21325643
- PMCID: PMC3094033
- DOI: 10.1152/ajpregu.91046.2008
High-end arteriolar resistance limits uterine artery blood flow and restricts fetal growth in preeclampsia and gestational hypertension at high altitude
Abstract
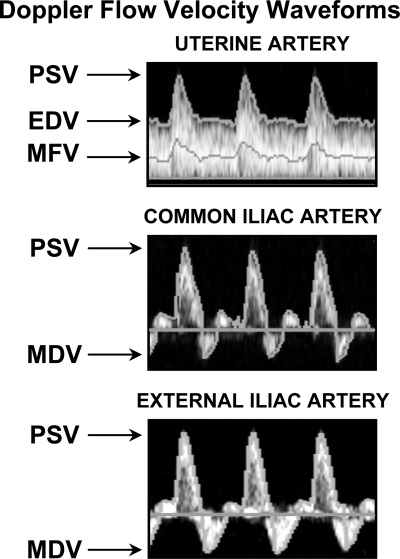
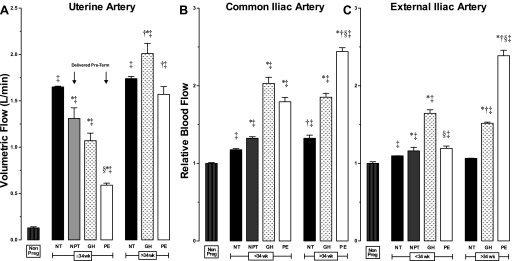
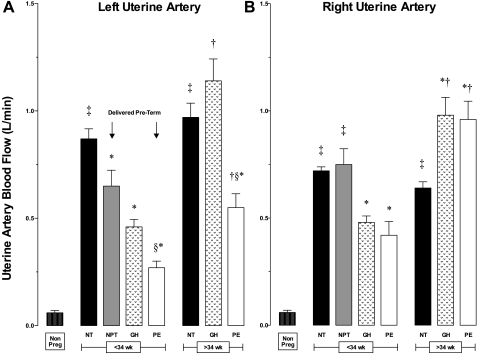
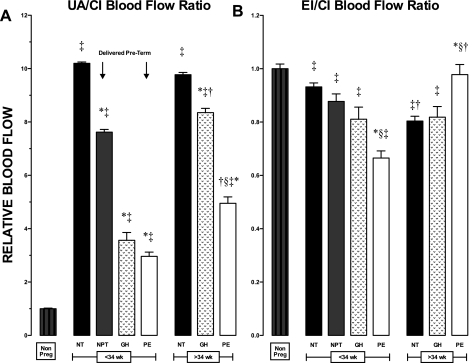
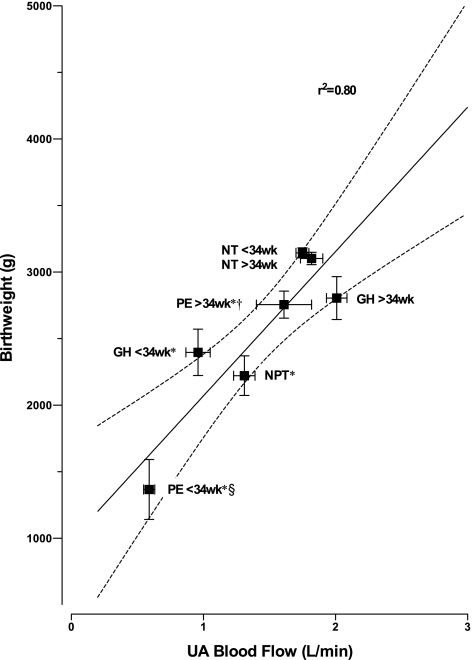
The reduction in infant birth weight and increased frequency of preeclampsia (PE) in high-altitude residents have been attributed to greater placental hypoxia, smaller uterine artery (UA) diameter, and lower UA blood flow (Q(UA)). This cross-sectional case-control study determined UA, common iliac (CI), and external iliac (EI) arterial blood flow in Andeans residing at 3,600-4,100 m, who were either nonpregnant (NP, n = 23), or experiencing normotensive pregnancies (NORM; n = 155), preeclampsia (PE, n = 20), or gestational hypertension (GH, n = 12). Pregnancy enlarged UA diameter to ~0.62 cm in all groups, but indices of end-arteriolar vascular resistance were higher in PE or GH than in NORM. Q(UA) was lower in early-onset (≤34 wk) PE or GH than in NORM, but was normal in late-onset (>34 wk) illness. Left Q(UA) was consistently greater than right in NORM, but the pattern reversed in PE. Although Q(CI) and Q(EI) were higher in PE and GH than NORM, the fraction of Q(CI) distributed to the UA was reduced 2- to 3-fold. Women with early-onset PE delivered preterm, and 43% had stillborn small for gestational age (SGA) babies. Those with GH and late-onset PE delivered at term but had higher frequencies of SGA babies (GH=50%, PE=46% vs. NORM=15%, both P < 0.01). Birth weight was strongly associated with reduced Q(UA) (R(2) = 0.80, P < 0.01), as were disease severity and adverse fetal outcomes. We concluded that high end-arteriolar resistance, not smaller UA diameter, limited Q(UA) and restricted fetal growth in PE and GH. These are, to our knowledge, the first quantitative measurements of Q(UA) and pelvic blood flow in early- vs. late-onset PE in high-altitude residents.
Figures
Similar articles
-
Soluble Endoglin and Uterine Artery Flow Doppler Ultrasonography as Markers of Progression to Preeclampsia in Women with Gestational Hypertension.Gynecol Obstet Invest. 2021;86(5):445-453. doi: 10.1159/000519371. Epub 2021 Oct 18. Gynecol Obstet Invest. 2021. PMID: 34662881
-
Use of placental growth factor and uterine artery doppler pulsatility index in pregnancies involving intrauterine fetal growth restriction or preeclampsia to predict perinatal outcomes.Gynecol Obstet Invest. 2015;80(2):99-105. doi: 10.1159/000370332. Epub 2015 Apr 22. Gynecol Obstet Invest. 2015. PMID: 25924544
-
Greater uterine artery blood flow during pregnancy in multigenerational (Andean) than shorter-term (European) high-altitude residents.Am J Physiol Regul Integr Comp Physiol. 2007 Sep;293(3):R1313-24. doi: 10.1152/ajpregu.00806.2006. Epub 2007 Jun 20. Am J Physiol Regul Integr Comp Physiol. 2007. PMID: 17581833
-
First-trimester uterine artery Doppler and adverse pregnancy outcome: a meta-analysis involving 55,974 women.Ultrasound Obstet Gynecol. 2014 May;43(5):500-7. doi: 10.1002/uog.13275. Epub 2014 Apr 4. Ultrasound Obstet Gynecol. 2014. PMID: 24339044 Review.
-
Uterine Artery Doppler in Screening for Preeclampsia and Fetal Growth Restriction.Rev Bras Ginecol Obstet. 2018 May;40(5):287-293. doi: 10.1055/s-0038-1660777. Epub 2018 Jun 18. Rev Bras Ginecol Obstet. 2018. PMID: 29913544 Free PMC article. Review.
Cited by
-
Ca2+-Activated K+ Channels and the Regulation of the Uteroplacental Circulation.Int J Mol Sci. 2023 Jan 10;24(2):1349. doi: 10.3390/ijms24021349. Int J Mol Sci. 2023. PMID: 36674858 Free PMC article. Review.
-
Long-term high altitude hypoxia during gestation suppresses large conductance Ca2+ -activated K+ channel function in uterine arteries: a causal role for microRNA-210.J Physiol. 2018 Dec;596(23):5891-5906. doi: 10.1113/JP276058. Epub 2018 Jul 1. J Physiol. 2018. PMID: 29869786 Free PMC article.
-
Internal iliac and uterine arteries Doppler ultrasound in the assessment of normotensive and chronic hypertensive pregnant women.Sci Rep. 2014 Jan 21;4:3785. doi: 10.1038/srep03785. Sci Rep. 2014. PMID: 24445576 Free PMC article.
-
Chronic binge alcohol consumption during pregnancy alters rat maternal uterine artery pressure response.Alcohol. 2016 Nov;56:59-64. doi: 10.1016/j.alcohol.2016.10.005. Epub 2016 Oct 13. Alcohol. 2016. PMID: 27793545 Free PMC article.
-
AMPK activation in pregnant human myometrial arteries from high-altitude and intrauterine growth-restricted pregnancies.Am J Physiol Heart Circ Physiol. 2020 Jul 1;319(1):H203-H212. doi: 10.1152/ajpheart.00644.2019. Epub 2020 Jun 5. Am J Physiol Heart Circ Physiol. 2020. PMID: 32502374 Free PMC article.
References
-
- Bosio P, McKenna P, Conroy R, O'Herlihy C. Maternal cental hemodynamics in hypertensive disorders of pregnancy. Obstet Gynecol 94: 978–984, 1999 - PubMed
-
- Bower S, Bewley S, Campbell S. Improved prediction of preecalmpsia by two-stage screeening of uterine arteries using the early diastolic notch and color Doppler imaging. Obstet Gynecol 82: 78–83, 1993 - PubMed
-
- Brosens IA, Robertson WB, Dixon HG. The role of the spiral arteries in the pathogenesis of preeclampsia. Obstet Gynecol Annu 1: 177–191, 1972 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous