

Autoimmune acute liver failure: proposed clinical and histological criteria
- PMID: 21274872
- PMCID: PMC3080034
- DOI: 10.1002/hep.24080
Autoimmune acute liver failure: proposed clinical and histological criteria
Abstract
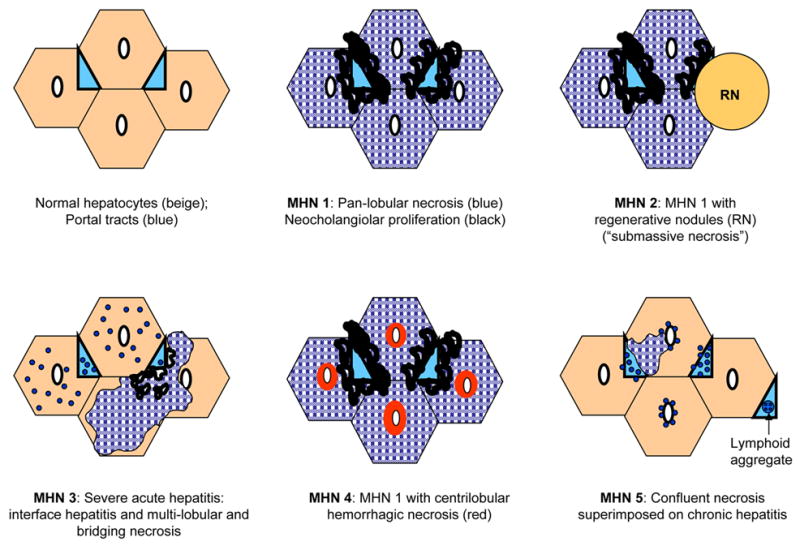
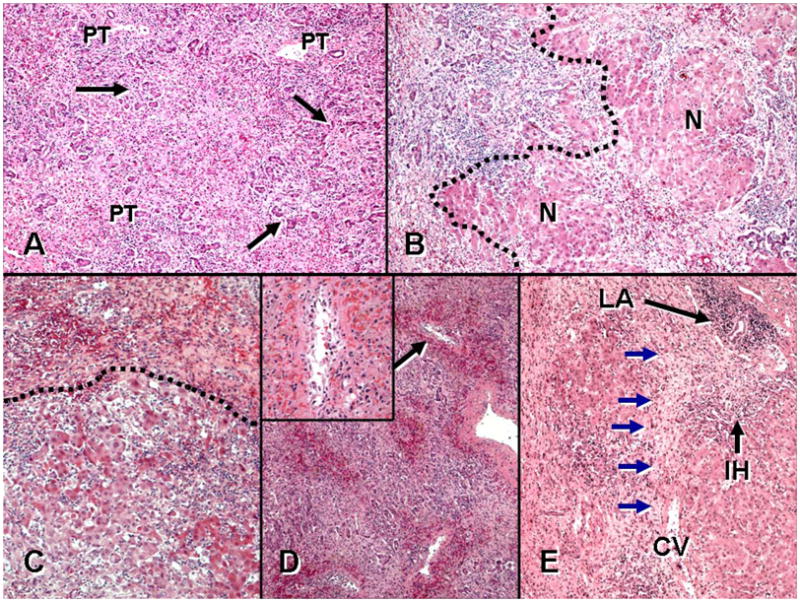
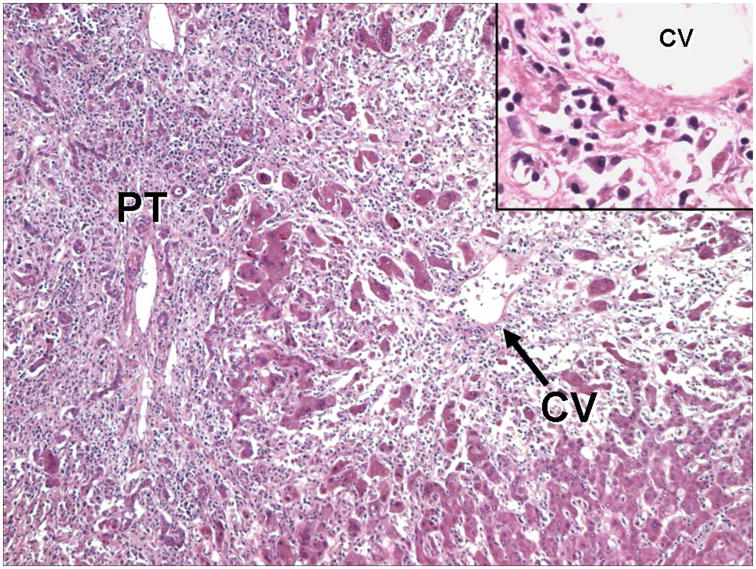
Identifying autoimmune hepatitis as the etiology of acute liver failure (ALF) is potentially important, because administering corticosteroids might avoid the need for liver transplantation. However, clinical and histological criteria of autoimmune ALF (AI-ALF) have not been defined. Liver sections (biopsies and explants) from a 72-patient subset of the ALF Study Group Registry with indeterminate ALF were reviewed by a pathologist blinded to all clinical data and were diagnosed with probable AI-ALF based on four features suggestive of an autoimmune pathogenesis: distinctive patterns of massive hepatic necrosis (present in 42% of sections), presence of lymphoid follicles (32%), a plasma cell-enriched inflammatory infiltrate (63%), and central perivenulitis (65%). Forty-two sections (58%) were considered probable for AI-ALF; this group demonstrated higher serum globulins (3.7 ± 0.2 g/dL versus 3.0 ± 0.2 g/dL; P = 0.037) and a higher prevalence of antinuclear and/or anti-smooth muscle antibodies (73% versus 48%; P = 0.034) compared to those without histology suggestive of probable AI-ALF. Thirty patients concordant for autoantibodies and probable AI-ALF upon histological analysis were more likely to have the classical autoimmune hepatitis phenotype (female predominance [72% versus 48%; P < 0.05], higher globulins [3.9 ± 0.2 g/dL versus 3.0 ± 0.2 g/dL; P < 0.005], and higher incidence of chronic hepatitis in long-term follow-up [67% versus 17%, P = 0.019]) compared to the population without concordant AI-ALF histology and autoantibodies.
Conclusion: Patients with indeterminate ALF often have features of autoimmune disease by histological analysis, serological testing, and clinical recurrence during follow-up. In contrast to classical autoimmune hepatitis, histological features of AI-ALF predominate in the centrilobular zone.
Copyright © 2010 American Association for the Study of Liver Diseases.
Figures
Comment in
-
Efforts at making the diagnosis of acute-onset autoimmune hepatitis.Hepatology. 2011 Jul;54(1):371-2; author reply 373. doi: 10.1002/hep.24331. Hepatology. 2011. PMID: 21452289 No abstract available.
-
Autoimmune acute liver failure.Hepatology. 2011 Jul;54(1):372-3; author reply 373. doi: 10.1002/hep.24337. Epub 2011 May 2. Hepatology. 2011. PMID: 21465508 No abstract available.
Similar articles
-
Acute liver failure histopathology: A 5-year retrospective study.Indian J Gastroenterol. 2024 Apr;43(2):468-474. doi: 10.1007/s12664-024-01588-0. Epub 2024 May 7. Indian J Gastroenterol. 2024. PMID: 38713344
-
Autoimmune acute liver failure and seronegative autoimmune liver disease in children: Are they different from classical disease?Eur J Gastroenterol Hepatol. 2017 Dec;29(12):1408-1415. doi: 10.1097/MEG.0000000000000975. Eur J Gastroenterol Hepatol. 2017. PMID: 28914695
-
Fulminant hepatic failure of autoimmune aetiology in children.J Pediatr Gastroenterol Nutr. 2015 Feb;60(2):159-64. doi: 10.1097/MPG.0000000000000593. J Pediatr Gastroenterol Nutr. 2015. PMID: 25304891
-
Acute presentation of autoimmune hepatitis -from acute hepatitis to ALF and ACLF.Hepatol Int. 2024 Oct;18(5):1385-1395. doi: 10.1007/s12072-024-10714-1. Epub 2024 Aug 11. Hepatol Int. 2024. PMID: 39127981 Review.
-
Re-analysis of clinical features of 89 patients with autoimmune hepatitis using the revised scoring system proposed by the International Autoimmune Hepatitis Group.Intern Med. 2000 Dec;39(12):1008-12. doi: 10.2169/internalmedicine.39.1008. Intern Med. 2000. PMID: 11197782 Review.
Cited by
-
Autoimmune hepatitis, one disease with many faces: etiopathogenetic, clinico-laboratory and histological characteristics.World J Gastroenterol. 2015 Jan 7;21(1):60-83. doi: 10.3748/wjg.v21.i1.60. World J Gastroenterol. 2015. PMID: 25574080 Free PMC article. Review.
-
Prevalence and Significance of Autoantibodies in Children With Acute Liver Failure.J Pediatr Gastroenterol Nutr. 2017 Feb;64(2):210-217. doi: 10.1097/MPG.0000000000001363. J Pediatr Gastroenterol Nutr. 2017. PMID: 27496798 Free PMC article.
-
Acute onset of autoimmune hepatitis with sinusoidal and central vein endotheliitis, and marked involvement of activated dendritic cells: A case report.Medicine (Baltimore). 2018 Dec;97(52):e13873. doi: 10.1097/MD.0000000000013873. Medicine (Baltimore). 2018. PMID: 30593193 Free PMC article.
-
The fingerprint of antimitochondrial antibodies and the etiology of primary biliary cholangitis.Hepatology. 2017 May;65(5):1670-1682. doi: 10.1002/hep.29059. Epub 2017 Mar 31. Hepatology. 2017. PMID: 28100006 Free PMC article.
-
Future directions in acute liver failure.Hepatology. 2023 Oct 1;78(4):1266-1289. doi: 10.1097/HEP.0000000000000458. Epub 2023 May 16. Hepatology. 2023. PMID: 37183883 Free PMC article. Review.
References
-
- Manns MP, Strassburg CP. Autoimmune hepatitis: clinical challenges. Gastroenterology. 2001;120:1502–1517. - PubMed
-
- Soloway RD, Summerskill WH, Baggenstoss AH, Geall MG, Gitnick GL, Elveback IR, et al. Clinical, biochemical, and histological remission of severe chronic active liver disease: a controlled study of treatments and early prognosis. Gastroenterology. 1972;63:820–833. - PubMed
-
- Alvarez F, Berg PA, Bianchi FB, Bianchi L, Burroughs AK, Cancado EL, et al. International Autoimmune Hepatitis Group Report: review of criteria for diagnosis of autoimmune hepatitis. J Hepatol. 1999;31:929–938. - PubMed
-
- Hennes EM, Zeniya M, Czaja AJ, Pares A, Dalekos GN, Krawitt EL, et al. Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology. 2008;48:169–176. - PubMed
-
- Lee WM. Etiologies of acute liver failure. Semin Liver Dis. 2008;28:142–152. - PubMed