

Cytokine/anti-cytokine therapy - novel treatments for asthma?
- PMID: 21232048
- PMCID: PMC3085870
- DOI: 10.1111/j.1476-5381.2011.01219.x
Cytokine/anti-cytokine therapy - novel treatments for asthma?
Abstract
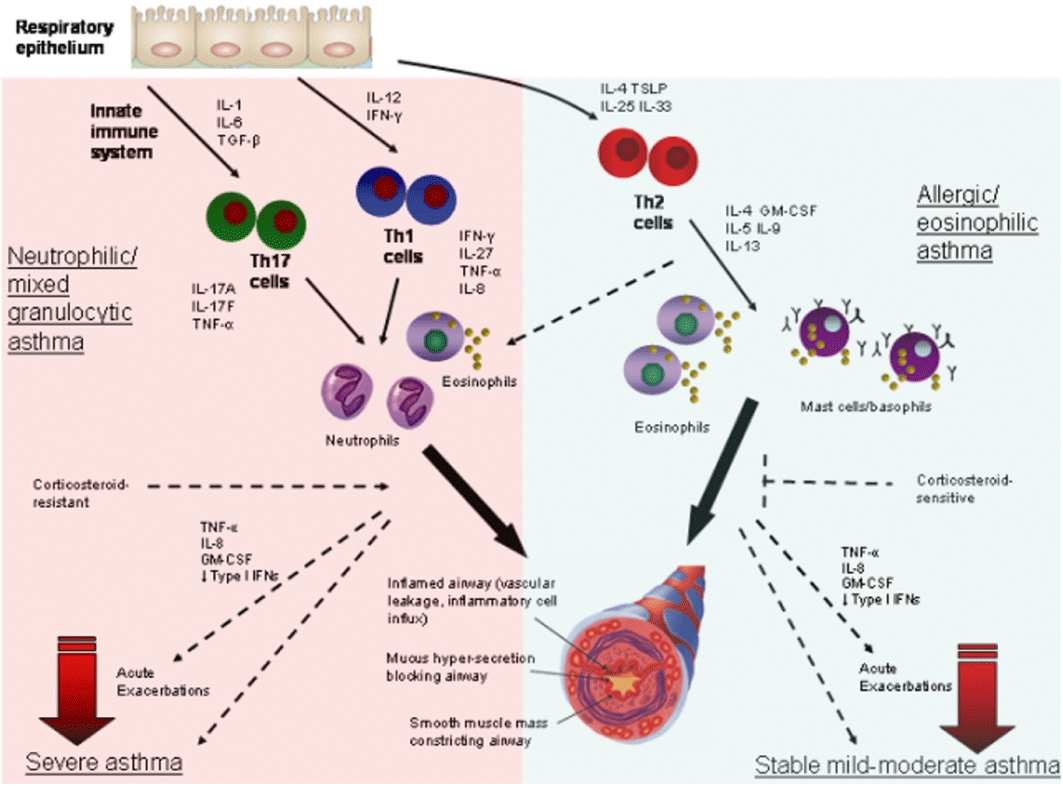
Asthma is a chronic inflammatory disease of the airways and there are no preventions or cures. Inflammatory cells through the secretion of cytokines and pro-inflammatory molecules are thought to play a critical role in pathogenesis. Type 2 CD4(+) lymphocytes (Th2 cells) and their cytokines predominate in mild to moderate allergic asthma, whereas severe steroid-resistant asthma has more of a mixed Th2/Th1 phenotype with a Th17 component. Other immune cells, particularly neutrophils, macrophages and dendritic cells, as well structural cells such as epithelial and airway smooth muscle cells also produce disease-associated cytokines in asthma. Increased levels of these immune cells and cytokines have been identified in clinical samples and their potential role in disease demonstrated in studies using mouse models of asthma. Clinical trials with inhibitors of cytokines such as interleukin (IL)-4, -5 and tumour necrosis factor-α have had success in some studies but not others. This may reflect the design of the clinical trials, including treatments regimes and the patient population included in these studies. IL-13, -9 and granulocyte-macrophage colony-stimulating factor are currently being evaluated in clinical trials or preclinically and the outcome of these studies is eagerly awaited. Roles for IL-25, -33, thymic stromal lymphopoietin, interferon-γ, IL-17 and -27 in the regulation of asthma are just emerging, identifying new ways to treat inflammation. Careful interpretation of results from mouse studies will inform the development and application of therapeutic approaches for asthma. The most effective approaches may be combination therapies that suppress multiple cytokines and a range of redundant and disconnected pathways that separately contribute to asthma pathogenesis. Astute application of these approaches may eventually lead to the development of effective asthma therapeutics. Here we review the current state of knowledge in the field.
© 2011 The Authors. British Journal of Pharmacology © 2011 The British Pharmacological Society.
Figures
Similar articles
-
New insights into the role of cytokines in asthma.J Clin Pathol. 2001 Aug;54(8):577-89. doi: 10.1136/jcp.54.8.577. J Clin Pathol. 2001. PMID: 11477111 Free PMC article. Review.
-
Inhibition of Bruton's tyrosine kinase and IL-2 inducible T-cell kinase suppresses both neutrophilic and eosinophilic airway inflammation in a cockroach allergen extract-induced mixed granulocytic mouse model of asthma using preventative and therapeutic strategy.Pharmacol Res. 2019 Oct;148:104441. doi: 10.1016/j.phrs.2019.104441. Epub 2019 Sep 7. Pharmacol Res. 2019. PMID: 31505252
-
Expression and Regulation of Thymic Stromal Lymphopoietin and Thymic Stromal Lymphopoietin Receptor Heterocomplex in the Innate-Adaptive Immunity of Pediatric Asthma.Int J Mol Sci. 2018 Apr 18;19(4):1231. doi: 10.3390/ijms19041231. Int J Mol Sci. 2018. PMID: 29670037 Free PMC article. Review.
-
Epidermal growth factor receptor signalling regulates granulocyte-macrophage colony-stimulating factor production by airway epithelial cells and established allergic airway disease.Clin Exp Allergy. 2016 Feb;46(2):317-28. doi: 10.1111/cea.12612. Clin Exp Allergy. 2016. PMID: 26263242 Free PMC article.
-
Protective Role of Eosinophils and TNFa after Ozone Inhalation.Res Rep Health Eff Inst. 2017 Mar;2017(191):1-41. Res Rep Health Eff Inst. 2017. PMID: 29659241 Free PMC article.
Cited by
-
ITGAM-macrophage modulation as a potential strategy for treating neutrophilic Asthma: insights from bioinformatics analysis and in vivo experiments.Apoptosis. 2024 Apr;29(3-4):393-411. doi: 10.1007/s10495-023-01914-5. Epub 2023 Nov 11. Apoptosis. 2024. PMID: 37950848
-
Chlamydia muridarum lung infection in infants alters hematopoietic cells to promote allergic airway disease in mice.PLoS One. 2012;7(8):e42588. doi: 10.1371/journal.pone.0042588. Epub 2012 Aug 1. PLoS One. 2012. PMID: 22870337 Free PMC article.
-
Investigation of the anti‑asthmatic activity of Oridonin on a mouse model of asthma.Mol Med Rep. 2016 Sep;14(3):2000-6. doi: 10.3892/mmr.2016.5485. Epub 2016 Jul 8. Mol Med Rep. 2016. PMID: 27431862 Free PMC article.
-
Extracellular Vesicles in Inner Ear Therapies-Pathophysiological, Manufacturing, and Clinical Considerations.J Clin Med. 2022 Dec 15;11(24):7455. doi: 10.3390/jcm11247455. J Clin Med. 2022. PMID: 36556073 Free PMC article. Review.
-
The link between atopic dermatitis and asthma- immunological imbalance and beyond.Asthma Res Pract. 2021 Dec 15;7(1):16. doi: 10.1186/s40733-021-00082-0. Asthma Res Pract. 2021. PMID: 34911576 Free PMC article. Review.
References
-
- Agache I, Ciobanu C, Agache C, Anghel M. Increased serum IL-17 is an independent risk factor for severe asthma. Respir Med. 2010;104:1131–1137. - PubMed
-
- Alcorn J, Crowe C, Kolls J. TH17 cells in asthma and COPD. Annu Rev Physiol. 2010;72:495–516. - PubMed
-
- Amrani Y, Moore P, Hoffman R, Shore S, Panettieri RJ. Interferon-gamma modulates cysteinyl leukotriene receptor-1 expression and function in human airway myocytes. Am J Respir Crit Care Med. 2001;1164:2098–2101. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
