

Phase III comparison of standard doxorubicin and cyclophosphamide versus weekly doxorubicin and daily oral cyclophosphamide plus granulocyte colony-stimulating factor as neoadjuvant therapy for inflammatory and locally advanced breast cancer: SWOG 0012
- PMID: 21220618
- PMCID: PMC3068051
- DOI: 10.1200/JCO.2009.27.6543
Phase III comparison of standard doxorubicin and cyclophosphamide versus weekly doxorubicin and daily oral cyclophosphamide plus granulocyte colony-stimulating factor as neoadjuvant therapy for inflammatory and locally advanced breast cancer: SWOG 0012
Abstract
Purpose: Patients with inflammatory breast cancer (IBC) or locally advanced breast cancer (LABC) were randomly assigned to 21-day doxorubicin and cyclophosphamide administered for five cycles (standard arm) versus weekly doxorubicin and daily oral cyclophosphamide administered with granulocyte colony-stimulating factor support for 15 weeks (continuous arm). All patients had subsequent weekly paclitaxel for 12 weeks before surgery.
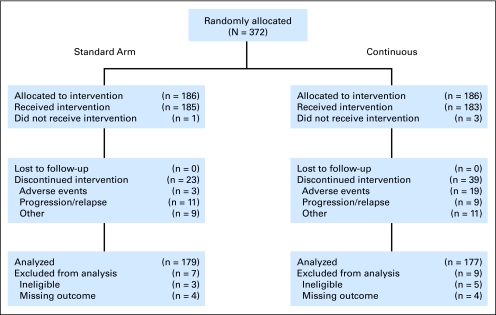
Patients and methods: Patients (n = 372) were randomly assigned to the standard arm (n = 186) or the continuous arm (n = 186) stratified by disease type (LABC, n = 256; IBC, n = 116). The primary outcome was microscopic pathologic complete response (pCR) at surgery. Secondary outcomes included disease-free survival, overall survival, and toxicity.
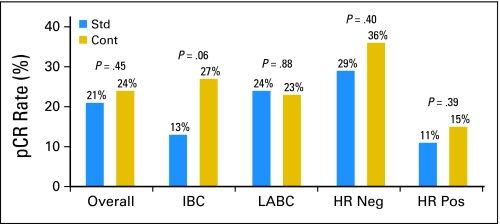
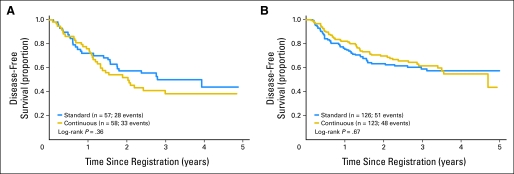
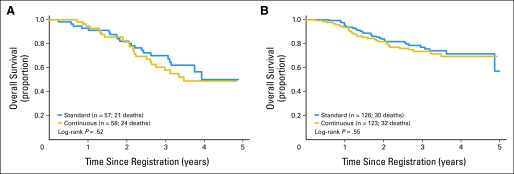
Results: More patients in the standard arm had grade 3 to 4 leukopenia and neutropenia, but there were more instances of stomatitis/pharyngitis and hand-foot skin reaction in the continuous arm. Assessed among 356 eligible patients, pCR was not different between the treatment groups stratified by disease type (P = .42). In subset analysis, higher pCR rates were observed in the continuous arm versus the standard arm only for stage IIIB disease (P = .0057) and in IBC (P = .06). Comparison of overall survival and disease-free survival showed no difference between treatment groups (P = .37 and P = .87, respectively).
Conclusion: No significant clinical benefit was seen for the investigational arm in this trial overall.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Similar articles
-
SWOG S0800 (NCI CDR0000636131): addition of bevacizumab to neoadjuvant nab-paclitaxel with dose-dense doxorubicin and cyclophosphamide improves pathologic complete response (pCR) rates in inflammatory or locally advanced breast cancer.Breast Cancer Res Treat. 2016 Aug;158(3):485-95. doi: 10.1007/s10549-016-3889-6. Epub 2016 Jul 8. Breast Cancer Res Treat. 2016. PMID: 27393622 Free PMC article. Clinical Trial.
-
Effects of the addition of gemcitabine, and paclitaxel-first sequencing, in neoadjuvant sequential epirubicin, cyclophosphamide, and paclitaxel for women with high-risk early breast cancer (Neo-tAnGo): an open-label, 2×2 factorial randomised phase 3 trial.Lancet Oncol. 2014 Feb;15(2):201-12. doi: 10.1016/S1470-2045(13)70554-0. Epub 2013 Dec 19. Lancet Oncol. 2014. PMID: 24360787 Clinical Trial.
-
Association of Stromal Tumor-Infiltrating Lymphocytes With Recurrence-Free Survival in the N9831 Adjuvant Trial in Patients With Early-Stage HER2-Positive Breast Cancer.JAMA Oncol. 2016 Jan;2(1):56-64. doi: 10.1001/jamaoncol.2015.3239. JAMA Oncol. 2016. PMID: 26469139 Free PMC article. Clinical Trial.
-
Lapatinib as a component of neoadjuvant therapy for HER2-positive operable breast cancer (NSABP protocol B-41): an open-label, randomised phase 3 trial.Lancet Oncol. 2013 Nov;14(12):1183-92. doi: 10.1016/S1470-2045(13)70411-X. Epub 2013 Oct 4. Lancet Oncol. 2013. PMID: 24095300 Clinical Trial.
-
Final results of a randomized phase III trial comparing cyclophosphamide, epirubicin, and fluorouracil with a dose-intensified epirubicin and cyclophosphamide + filgrastim as neoadjuvant treatment in locally advanced breast cancer: an EORTC-NCIC-SAKK multicenter study.J Clin Oncol. 2003 Mar 1;21(5):843-50. doi: 10.1200/JCO.2003.05.135. J Clin Oncol. 2003. PMID: 12610183 Review.
Cited by
-
Tumor metabolism and blood flow as assessed by positron emission tomography varies by tumor subtype in locally advanced breast cancer.Clin Cancer Res. 2010 May 15;16(10):2803-10. doi: 10.1158/1078-0432.CCR-10-0026. Epub 2010 May 11. Clin Cancer Res. 2010. PMID: 20460489 Free PMC article.
-
Prognostic impact of human epidermal growth factor-like receptor 2 and hormone receptor status in inflammatory breast cancer (IBC): analysis of 2,014 IBC patient cases from the California Cancer Registry.Breast Cancer Res. 2009;11(1):R9. doi: 10.1186/bcr2225. Epub 2009 Feb 19. Breast Cancer Res. 2009. PMID: 19228416 Free PMC article.
-
Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer: ASCO Guideline.J Clin Oncol. 2021 May 1;39(13):1485-1505. doi: 10.1200/JCO.20.03399. Epub 2021 Jan 28. J Clin Oncol. 2021. PMID: 33507815 Free PMC article.
-
Neoadjuvant therapy for locally advanced breast cancer: Focus on chemotherapy and biological targeted treatments' armamentarium.J Thorac Dis. 2010 Sep;2(3):160-70. doi: 10.3978/j.issn.2072-1439.2010.02.03.8. J Thorac Dis. 2010. PMID: 22263038 Free PMC article.
-
Similar response profile to neoadjuvant chemotherapy, but different survival, in inflammatory versus locally advanced breast cancers.Oncotarget. 2017 Jul 31;8(39):66019-66032. doi: 10.18632/oncotarget.19732. eCollection 2017 Sep 12. Oncotarget. 2017. PMID: 29029489 Free PMC article.
References
-
- Hryniuk W, Bush H. The importance of dose intensity in chemotherapy of metastatic breast cancer. J Clin Oncol. 1984;2:1281–1288. - PubMed
-
- Hryniuk WM, Levine MN, Levin L. Analysis of dose intensity for chemotherapy in early (stage II) and advanced breast cancer. NCI Monogr. 1986;1:87–94. - PubMed
-
- Hryniuk W, Levine MN. Analysis of dose intensity for adjuvant chemotherapy trials in stage II breast cancer. J Clin Oncol. 1986;4:1162–1170. - PubMed
-
- Ellis GK, Livingston RB, Gralow JR, et al. Dose-dense anthracycline-based chemotherapy for node-positive breast cancer. J Clin Oncol. 2002;20:3637–3643. - PubMed
-
- Ellis G, Green S, Livingston R, et al. Neoadjuvant doxorubicin, cyclophosphamide and G-CSF (AC+G) for locally advanced breast cancer (LABC), a Southwest Oncology Group phase II study. Proc Am Soc Clin Oncol. 2000;19(suppl):85a. abstr 326.
Publication types
MeSH terms
Substances
Grants and funding
- CA22433/CA/NCI NIH HHS/United States
- U10 CA035192/CA/NCI NIH HHS/United States
- U10 CA045808/CA/NCI NIH HHS/United States
- CA35281/CA/NCI NIH HHS/United States
- CA63845/CA/NCI NIH HHS/United States
- N01 CA046441/CA/NCI NIH HHS/United States
- U10 CA035178/CA/NCI NIH HHS/United States
- CA76447/CA/NCI NIH HHS/United States
- U10 CA032102/CA/NCI NIH HHS/United States
- U10 CA063844/CA/NCI NIH HHS/United States
- N01 CA004919/CA/NCI NIH HHS/United States
- CA379891/CA/NCI NIH HHS/United States
- CA86780/CA/NCI NIH HHS/United States
- N01 CA035176/CA/NCI NIH HHS/United States
- CA76462/CA/NCI NIH HHS/United States
- CA46136/CA/NCI NIH HHS/United States
- CA35128/CA/NCI NIH HHS/United States
- U10 CA004919/CA/NCI NIH HHS/United States
- N01 CA035431/CA/NCI NIH HHS/United States
- U10 CA045560/CA/NCI NIH HHS/United States
- CA12644/CA/NCI NIH HHS/United States
- U10 CA035128/CA/NCI NIH HHS/United States
- CA20319/CA/NCI NIH HHS/United States
- U10 CA063845/CA/NCI NIH HHS/United States
- N01 CA032102/CA/NCI NIH HHS/United States
- U10 CA014028/CA/NCI NIH HHS/United States
- N01 CA035119/CA/NCI NIH HHS/United States
- CA45808/CA/NCI NIH HHS/United States
- CA14028/CA/NCI NIH HHS/United States
- CA58882/CA/NCI NIH HHS/United States
- CA45377/CA/NCI NIH HHS/United States
- U10 CA074647/CA/NCI NIH HHS/United States
- U10 CA035281/CA/NCI NIH HHS/United States
- CA11083/CA/NCI NIH HHS/United States
- CA58861/CA/NCI NIH HHS/United States
- CA35090/CA/NCI NIH HHS/United States
- N01 CA063844/CA/NCI NIH HHS/United States
- CA46282/CA/NCI NIH HHS/United States
- U10 CA046282/CA/NCI NIH HHS/United States
- N01 CA035178/CA/NCI NIH HHS/United States
- N01 CA038926/CA/NCI NIH HHS/United States
- U10 CA067575/CA/NCI NIH HHS/United States
- CA74811/CA/NCI NIH HHS/United States
- U10 CA046441/CA/NCI NIH HHS/United States
- U10 CA045377/CA/NCI NIH HHS/United States
- CA35192/CA/NCI NIH HHS/United States
- U10 CA058882/CA/NCI NIH HHS/United States
- CA74647/CA/NCI NIH HHS/United States
- U10 CA020319/CA/NCI NIH HHS/United States
- U10 CA038926/CA/NCI NIH HHS/United States
- CA76448/CA/NCI NIH HHS/United States
- U10 CA086780/CA/NCI NIH HHS/United States
- U10 CA074811/CA/NCI NIH HHS/United States
- U10 CA035431/CA/NCI NIH HHS/United States
- U10 CA035119/CA/NCI NIH HHS/United States
- U10 CA095860/CA/NCI NIH HHS/United States
- U10 CA011083/CA/NCI NIH HHS/United States
- CA52654/CA/NCI NIH HHS/United States
- N01 CA067575/CA/NCI NIH HHS/United States
- U10 CA052654/CA/NCI NIH HHS/United States
- U10 CA035176/CA/NCI NIH HHS/United States
- U10 CA035090/CA/NCI NIH HHS/United States
- CA95860/CA/NCI NIH HHS/United States
- U10 CA058861/CA/NCI NIH HHS/United States
- N01 CA045560/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
