

Cancer survival in Australia, Canada, Denmark, Norway, Sweden, and the UK, 1995-2007 (the International Cancer Benchmarking Partnership): an analysis of population-based cancer registry data
- PMID: 21183212
- PMCID: PMC3018568
- DOI: 10.1016/S0140-6736(10)62231-3
Cancer survival in Australia, Canada, Denmark, Norway, Sweden, and the UK, 1995-2007 (the International Cancer Benchmarking Partnership): an analysis of population-based cancer registry data
Abstract
Background: Cancer survival is a key measure of the effectiveness of health-care systems. Persistent regional and international differences in survival represent many avoidable deaths. Differences in survival have prompted or guided cancer control strategies. This is the first study in a programme to investigate international survival disparities, with the aim of informing health policy to raise standards and reduce inequalities in survival.
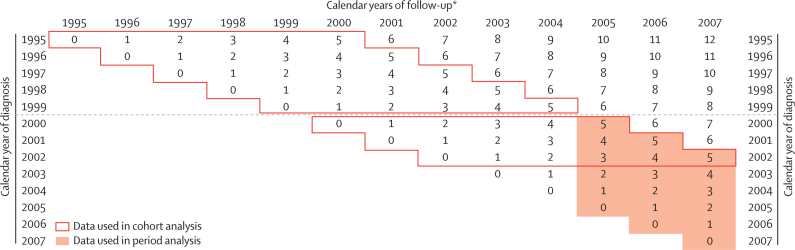
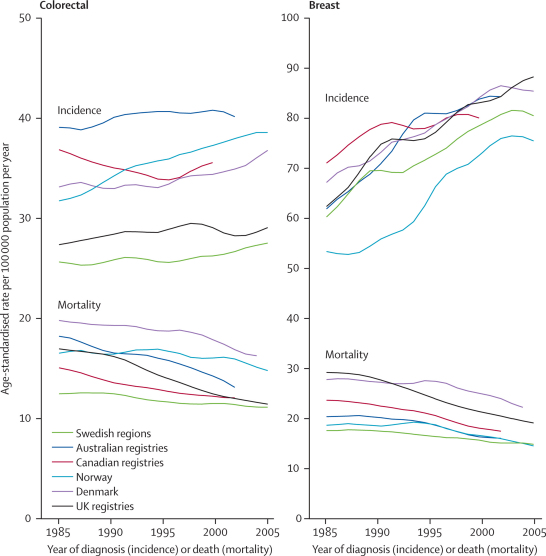
Methods: Data from population-based cancer registries in 12 jurisdictions in six countries were provided for 2·4 million adults diagnosed with primary colorectal, lung, breast (women), or ovarian cancer during 1995-2007, with follow-up to Dec 31, 2007. Data quality control and analyses were done centrally with a common protocol, overseen by external experts. We estimated 1-year and 5-year relative survival, constructing 252 complete life tables to control for background mortality by age, sex, and calendar year. We report age-specific and age-standardised relative survival at 1 and 5 years, and 5-year survival conditional on survival to the first anniversary of diagnosis. We also examined incidence and mortality trends during 1985-2005.
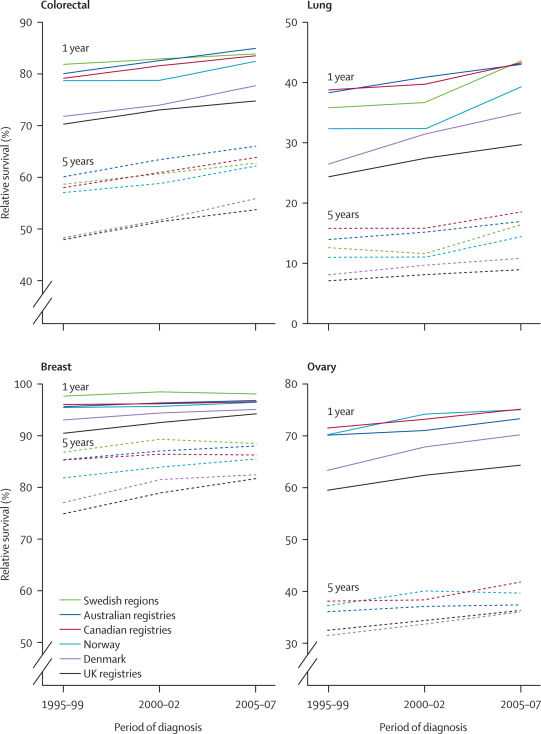
Findings: Relative survival improved during 1995-2007 for all four cancers in all jurisdictions. Survival was persistently higher in Australia, Canada, and Sweden, intermediate in Norway, and lower in Denmark, England, Northern Ireland, and Wales, particularly in the first year after diagnosis and for patients aged 65 years and older. International differences narrowed at all ages for breast cancer, from about 9% to 5% at 1 year and from about 14% to 8% at 5 years, but less or not at all for the other cancers. For colorectal cancer, the international range narrowed only for patients aged 65 years and older, by 2-6% at 1 year and by 2-3% at 5 years.
Interpretation: Up-to-date survival trends show increases but persistent differences between countries. Trends in cancer incidence and mortality are broadly consistent with these trends in survival. Data quality and changes in classification are not likely explanations. The patterns are consistent with later diagnosis or differences in treatment, particularly in Denmark and the UK, and in patients aged 65 years and older.
Funding: Department of Health, England; and Cancer Research UK.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Caution needed for country-specific cancer survival.Lancet. 2011 Jan 8;377(9760):99-101. doi: 10.1016/S0140-6736(10)62347-1. Lancet. 2011. PMID: 21215872 No abstract available.
-
Cancer survival in Australia, Canada, Denmark, Norway, Sweden, and the UK.Lancet. 2011 Apr 2;377(9772):1149; author reply 1149-50. doi: 10.1016/S0140-6736(11)60456-X. Lancet. 2011. PMID: 21459201 No abstract available.
-
Cancer survival in Australia, Canada, Denmark, Norway, Sweden, and the UK.Lancet. 2011 Apr 2;377(9772):1149; author reply 1149-50. doi: 10.1016/S0140-6736(11)60455-8. Lancet. 2011. PMID: 21459202 No abstract available.
Similar articles
-
Progress in cancer survival, mortality, and incidence in seven high-income countries 1995-2014 (ICBP SURVMARK-2): a population-based study.Lancet Oncol. 2019 Nov;20(11):1493-1505. doi: 10.1016/S1470-2045(19)30456-5. Epub 2019 Sep 11. Lancet Oncol. 2019. PMID: 31521509 Free PMC article.
-
Explaining variation in cancer survival between 11 jurisdictions in the International Cancer Benchmarking Partnership: a primary care vignette survey.BMJ Open. 2015 May 27;5(5):e007212. doi: 10.1136/bmjopen-2014-007212. BMJ Open. 2015. PMID: 26017370 Free PMC article.
-
International variation in childhood cancer mortality rates from 2001 to 2015: Comparison of trends in the International Cancer Benchmarking Partnership countries.Int J Cancer. 2022 Jan 1;150(1):28-37. doi: 10.1002/ijc.33774. Epub 2021 Oct 7. Int J Cancer. 2022. PMID: 34449879
-
Comparability of stage data in cancer registries in six countries: lessons from the International Cancer Benchmarking Partnership.Int J Cancer. 2013 Feb 1;132(3):676-85. doi: 10.1002/ijc.27651. Epub 2012 Jun 28. Int J Cancer. 2013. PMID: 22623157
-
Paediatric cancer stage in population-based cancer registries: the Toronto consensus principles and guidelines.Lancet Oncol. 2016 Apr;17(4):e163-e172. doi: 10.1016/S1470-2045(15)00539-2. Epub 2016 Mar 29. Lancet Oncol. 2016. PMID: 27300676 Review.
Cited by
-
The role of primary care in cancer diagnosis via emergency presentation: qualitative synthesis of significant event reports.Br J Cancer. 2015 Mar 31;112 Suppl 1(Suppl 1):S50-6. doi: 10.1038/bjc.2015.42. Br J Cancer. 2015. PMID: 25734395 Free PMC article.
-
A novel blood based triage test for colorectal cancer in primary care: a pilot study.BJGP Open. 2023 Mar 21;7(1):BJGPO.2022.0077. doi: 10.3399/BJGPO.2022.0077. Print 2023 Mar. BJGP Open. 2023. PMID: 36332909 Free PMC article.
-
Conditional survival in Canada: adjusting patient prognosis over time.Curr Oncol. 2012 Aug;19(4):222-4. doi: 10.3747/co.19.1148. Curr Oncol. 2012. PMID: 22876149 Free PMC article. No abstract available.
-
Evaluating the Educational Value of Cancer Registries - a Systematic Review and Thematic Analysis.J Cancer Educ. 2024 Apr;39(2):194-203. doi: 10.1007/s13187-023-02394-6. Epub 2023 Dec 26. J Cancer Educ. 2024. PMID: 38146032 Review.
-
Survival Rate of Colorectal Cancer in Eastern Mediterranean Region Countries: A Systematic Review and Meta-Analysis.Cancer Control. 2020 Jan-Dec;27(1):1073274820964146. doi: 10.1177/1073274820964146. Cancer Control. 2020. PMID: 33074714 Free PMC article.
References
-
- Coleman MP, Quaresma M, Berrino F, the CONCORD Working Group Cancer survival in five continents: a worldwide population-based study (CONCORD) Lancet Oncol. 2008;9:730–756. - PubMed
-
- Berrino F, De Angelis R, Sant M, the EUROCARE Working Group Survival for eight major cancers and all cancers combined for European adults diagnosed in 1995–99: results of the EUROCARE-4 study. Lancet Oncol. 2007;8:773–783. - PubMed
-
- Berrino F, Sant M, Verdecchia A, editors. Survival of cancer patients in Europe: the EUROCARE study (IARC Scientific Publications number 132) International Agency for Research on Cancer; Lyon: 1995.
-
- Berrino F, Capocaccia R, Estève J, editors. Survival of cancer patients in Europe: the EUROCARE-2 study (IARC Scientific Publications number 151) International Agency for Research on Cancer; Lyon: 1999. - PubMed
-
- Sant M, Aareleid T, Berrino F. EUROCARE-3: survival of cancer patients diagnosed 1990–94—results and commentary. Ann Oncol. 2003;14(suppl 5):61–118. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
