

Metabolomic characterization of human prostate cancer bone metastases reveals increased levels of cholesterol
- PMID: 21151972
- PMCID: PMC2997052
- DOI: 10.1371/journal.pone.0014175
Metabolomic characterization of human prostate cancer bone metastases reveals increased levels of cholesterol
Abstract
Background: Metastasis to the bone is one clinically important features of prostate cancer (PCa). Current diagnostic methods cannot predict metastatic PCa at a curable stage of the disease. Identification of metabolic pathways involved in the growth of bone metastases therefore has the potential to improve PCa prognostication as well as therapy.
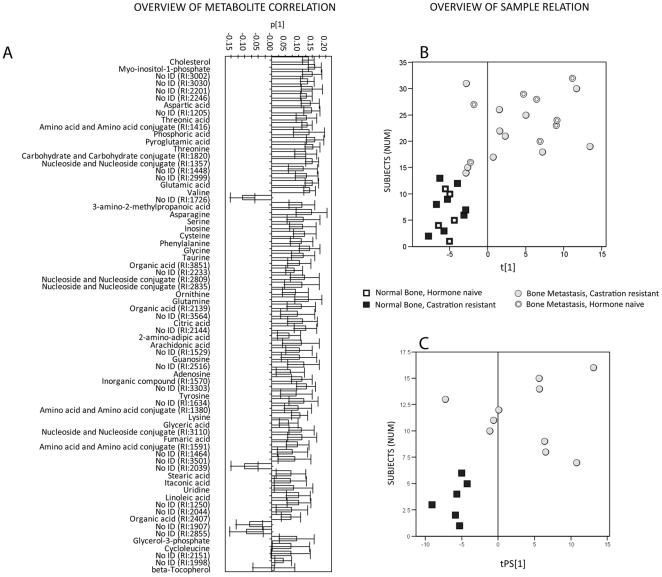
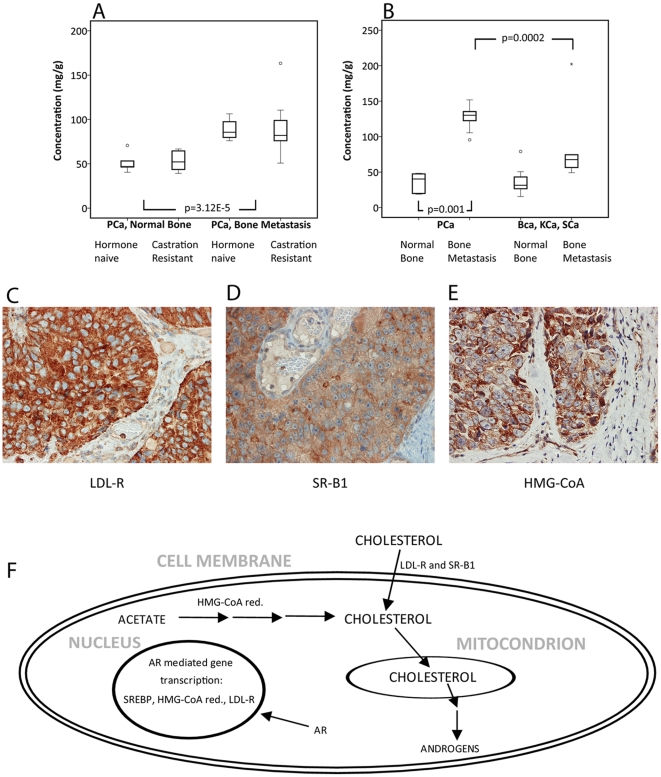
Methodology/principal findings: Metabolomics was applied for the study of PCa bone metastases (n = 20) in comparison with corresponding normal bone (n = 14), and furthermore of malignant (n = 13) and benign (n = 17) prostate tissue and corresponding plasma samples obtained from patients with (n = 15) and without (n = 13) diagnosed metastases and from men with benign prostate disease (n = 30). This was done using gas chromatography-mass spectrometry for sample characterization, and chemometric bioinformatics for data analysis. Results were verified in a separate test set including metastatic and normal bone tissue from patients with other cancers (n = 7). Significant differences were found between PCa bone metastases, bone metastases of other cancers, and normal bone. Furthermore, we identified metabolites in primary tumor tissue and in plasma which were significantly associated with metastatic disease. Among the metabolites in PCa bone metastases especially cholesterol was noted. In a test set the mean cholesterol level in PCa bone metastases was 127.30 mg/g as compared to 81.06 and 35.85 mg/g in bone metastases of different origin and normal bone, respectively (P = 0.0002 and 0.001). Immunohistochemical staining of PCa bone metastases showed intense staining of the low density lipoprotein receptor and variable levels of the scavenger receptor class B type 1 and 3-hydroxy-3-methylglutaryl-coenzyme reductase in tumor epithelial cells, indicating possibilities for influx and de novo synthesis of cholesterol.
Conclusions/significance: We have identified metabolites associated with PCa metastasis and specifically identified high levels of cholesterol in PCa bone metastases. Based on our findings and the previous literature, this makes cholesterol a possible therapeutic target for advanced PCa.
Conflict of interest statement
Figures

Similar articles
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Plasma metabolomic profile in prostatic intraepithelial neoplasia and prostate cancer and associations with the prostate-specific antigen and the Gleason score.Metabolomics. 2020 Jun 17;16(7):74. doi: 10.1007/s11306-020-01694-y. Metabolomics. 2020. PMID: 32556743
-
Integration of tissue metabolomics, transcriptomics and immunohistochemistry reveals ERG- and gleason score-specific metabolomic alterations in prostate cancer.Oncotarget. 2016 Jan 12;7(2):1421-38. doi: 10.18632/oncotarget.6370. Oncotarget. 2016. PMID: 26623558 Free PMC article.
-
Translational Metabolomics of Head Injury: Exploring Dysfunctional Cerebral Metabolism with Ex Vivo NMR Spectroscopy-Based Metabolite Quantification.In: Kobeissy FH, editor. Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects. Boca Raton (FL): CRC Press/Taylor & Francis; 2015. Chapter 25. In: Kobeissy FH, editor. Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects. Boca Raton (FL): CRC Press/Taylor & Francis; 2015. Chapter 25. PMID: 26269925 Free Books & Documents. Review.
-
Prostate cancer diagnosis and characterization with mass spectrometry imaging.Prostate Cancer Prostatic Dis. 2018 Sep;21(3):297-305. doi: 10.1038/s41391-017-0011-z. Epub 2017 Dec 5. Prostate Cancer Prostatic Dis. 2018. PMID: 29209003 Free PMC article. Review.
Cited by
-
Pseudouridine as a novel biomarker in prostate cancer.Urol Oncol. 2021 Jan;39(1):63-71. doi: 10.1016/j.urolonc.2020.06.026. Epub 2020 Jul 22. Urol Oncol. 2021. PMID: 32712138 Free PMC article. Review.
-
Farnesoid X Receptor Overexpression Decreases the Migration, Invasion and Angiogenesis of Human Bladder Cancers via AMPK Activation and Cholesterol Biosynthesis Inhibition.Cancers (Basel). 2022 Sep 9;14(18):4398. doi: 10.3390/cancers14184398. Cancers (Basel). 2022. PMID: 36139556 Free PMC article.
-
Preoperative plasma fatty acid metabolites inform risk of prostate cancer progression and may be used for personalized patient stratification.BMC Cancer. 2019 Dec 16;19(1):1216. doi: 10.1186/s12885-019-6418-2. BMC Cancer. 2019. PMID: 31842810 Free PMC article.
-
Tumor-intrinsic metabolic reprogramming and how it drives resistance to anti-PD-1/PD-L1 treatment.Cancer Drug Resist. 2023 Sep 4;6(3):611-641. doi: 10.20517/cdr.2023.60. eCollection 2023. Cancer Drug Resist. 2023. PMID: 37842241 Free PMC article. Review.
-
Global Prioritization of Disease Candidate Metabolites Based on a Multi-omics Composite Network.Sci Rep. 2015 Nov 24;5:17201. doi: 10.1038/srep17201. Sci Rep. 2015. PMID: 26598063 Free PMC article.
References
-
- Catalona WJ, Partin AW, Slawin KM, Brawer MK, Flanigan RC, et al. Use of the percentage of free prostate-specific antigen to enhance differentiation of prostate cancer from benign prostatic disease: a prospective multicenter clinical trial. JAMA. 1998;279:1542–1547. - PubMed
-
- Klotz L. Active surveillance versus radical treatment for favorable-risk localized prostate cancer. Curr Treat Options Oncol. 2006;7:355–362. - PubMed
-
- Lopergolo A, Zaffaroni N. Biomolecular markers of outcome prediction in prostate cancer. Cancer. 2009;115:3058–3067. - PubMed
-
- Parekh DJ, Ankerst DP, Troyer D, Srivastava S, Thompson IM. Biomarkers for prostate cancer detection. J Urol. 2007;178:2252–2259. - PubMed
-
- Fowler AH, Pappas AA, Holder JC, Finkbeiner AE, Dalrymple GV, et al. Differentiation of human prostate cancer from benign hypertrophy by in vitro 1H NMR. Magn Reson Med. 1992;25:140–147. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
