

Severe pandemic 2009 H1N1 influenza disease due to pathogenic immune complexes
- PMID: 21131958
- PMCID: PMC3034774
- DOI: 10.1038/nm.2262
Severe pandemic 2009 H1N1 influenza disease due to pathogenic immune complexes
Abstract
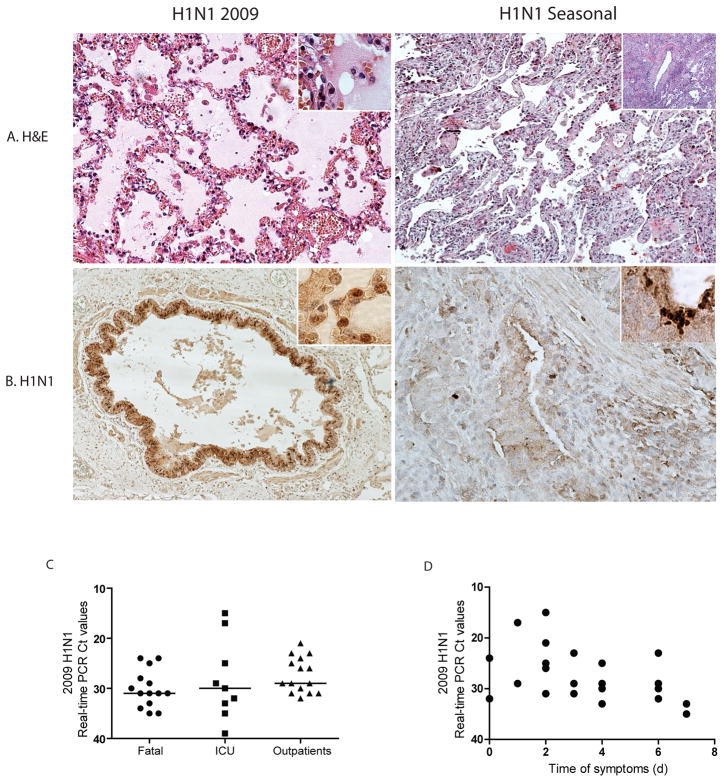
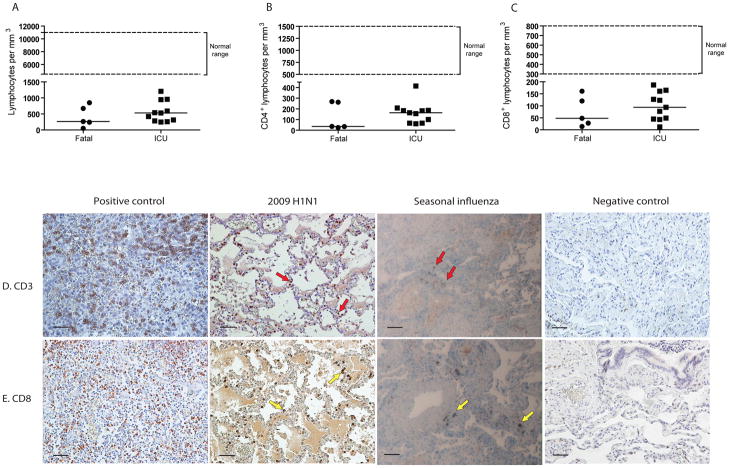
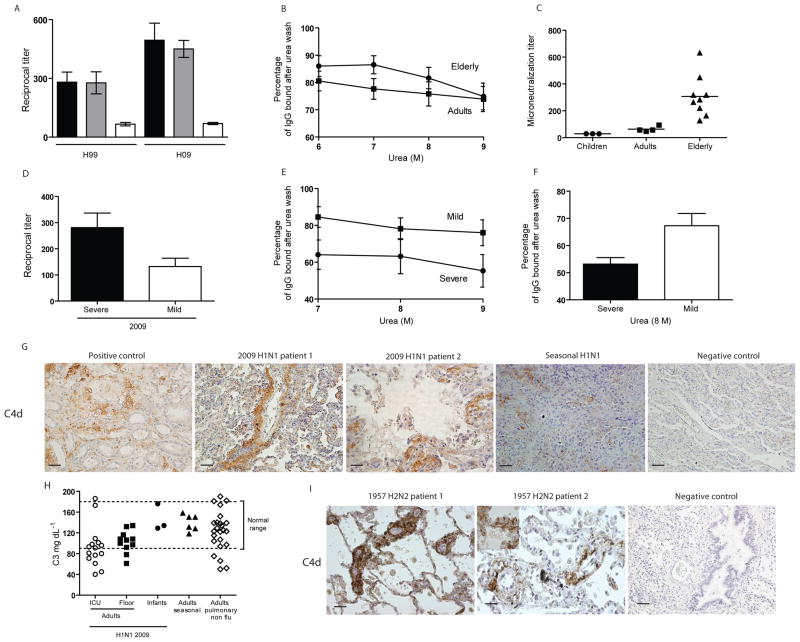
Pandemic influenza viruses often cause severe disease in middle-aged adults without preexisting comorbidities. The mechanism of illness associated with severe disease in this age group is not well understood. Here we find preexisting serum antibodies that cross-react with, but do not protect against, 2009 H1N1 influenza virus in middle-aged adults. Nonprotective antibody is associated with immune complex-mediated disease after infection. We detected high titers of serum antibody of low avidity for H1-2009 antigen, and low-avidity pulmonary immune complexes against the same protein, in severely ill individuals. Moreover, C4d deposition--a marker of complement activation mediated by immune complexes--was present in lung sections of fatal cases. Archived lung sections from middle-aged adults with confirmed fatal influenza 1957 H2N2 infection revealed a similar mechanism of illness. These observations provide a previously unknown biological mechanism for the unusual age distribution of severe cases during influenza pandemics.
Figures

Similar articles
-
Serum strain-specific or cross-reactive neuraminidase inhibiting antibodies against pandemic А/California/07/2009(H1N1) influenza in healthy volunteers.BMC Res Notes. 2015 Apr 10;8:136. doi: 10.1186/s13104-015-1086-z. BMC Res Notes. 2015. PMID: 25889924 Free PMC article.
-
Cytokine and chemokine profiles in lung tissues from fatal cases of 2009 pandemic influenza A (H1N1): role of the host immune response in pathogenesis.Am J Pathol. 2013 Oct;183(4):1258-1268. doi: 10.1016/j.ajpath.2013.06.023. Epub 2013 Aug 11. Am J Pathol. 2013. PMID: 23938324 Free PMC article.
-
Cross-reactive immunity against influenza viruses in children and adults following 2009 pandemic H1N1 infection.Antiviral Res. 2015 Feb;114:106-12. doi: 10.1016/j.antiviral.2014.12.008. Epub 2014 Dec 13. Antiviral Res. 2015. PMID: 25513756
-
Assessment of baseline age-specific antibody prevalence and incidence of infection to novel influenza A/H1N1 2009.Health Technol Assess. 2010 Dec;14(55):115-92. doi: 10.3310/hta14550-03. Health Technol Assess. 2010. PMID: 21208549
-
Age-associated cross-reactive antibody-dependent cellular cytotoxicity toward 2009 pandemic influenza A virus subtype H1N1.J Infect Dis. 2013 Oct 1;208(7):1051-61. doi: 10.1093/infdis/jit294. Epub 2013 Jun 28. J Infect Dis. 2013. PMID: 23812238
Cited by
-
What was the cause of the epidemic in Savannah in 1733?J R Soc Med. 2014 Dec;107(12):468-73. doi: 10.1177/0141076813486466. Epub 2013 May 28. J R Soc Med. 2014. PMID: 23759890 Free PMC article. No abstract available.
-
Sociodemographic factors and clinical conditions associated to hospitalization in influenza A (H1N1) 2009 virus infected patients in Spain, 2009-2010.PLoS One. 2012;7(3):e33139. doi: 10.1371/journal.pone.0033139. Epub 2012 Mar 7. PLoS One. 2012. PMID: 22412995 Free PMC article.
-
What Do Chaotrope-Based Avidity Assays for Antibodies to HIV-1 Envelope Glycoproteins Measure?J Virol. 2015 Jun;89(11):5981-95. doi: 10.1128/JVI.00320-15. Epub 2015 Mar 25. J Virol. 2015. PMID: 25810537 Free PMC article.
-
Fc-Effector-Independent in vivo Activity of a Potent Influenza B Neuraminidase Broadly Neutralizing Antibody.Viruses. 2023 Jul 13;15(7):1540. doi: 10.3390/v15071540. Viruses. 2023. PMID: 37515226 Free PMC article.
-
Immune Imprinting in the Influenza Ferret Model.Vaccines (Basel). 2020 Apr 8;8(2):173. doi: 10.3390/vaccines8020173. Vaccines (Basel). 2020. PMID: 32276530 Free PMC article. Review.
References
-
- Tumpey TM, et al. Characterization of the Reconstructed 1918 Spanish Influenza Pandemic Virus. Science. 2005;310:77–80. - PubMed
-
- Kobasa D, et al. Aberrant innate immune response in lethal infection of macaques with the 1918 influenza virus. Nature. 2007;445:319–323. - PubMed
-
- Geiss GK, et al. Cellular transcriptional profiling in influenza A virus-infected lung epithelial cells: the role of the nonstructural NS1 protein in the evasion of the host innate defense and its potential contribution to pandemic influenza. Proc Natl Acad Sci USA. 2002;99:10736–10741. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
