

Targeted therapy for high-grade glioma with the TGF-β2 inhibitor trabedersen: results of a randomized and controlled phase IIb study
- PMID: 20980335
- PMCID: PMC3018908
- DOI: 10.1093/neuonc/noq142
Targeted therapy for high-grade glioma with the TGF-β2 inhibitor trabedersen: results of a randomized and controlled phase IIb study
Abstract
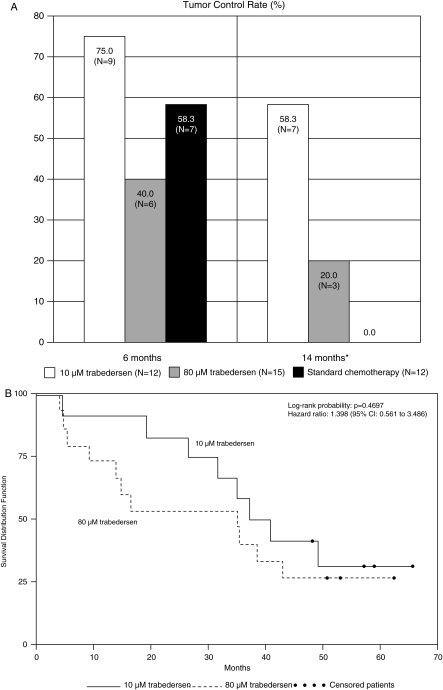
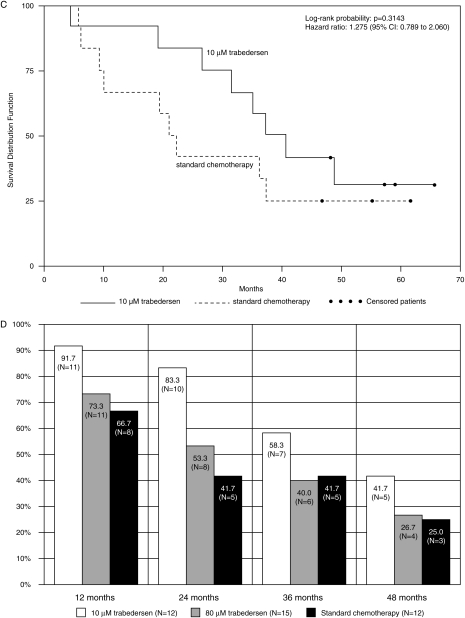
This randomized, open-label, active-controlled, dose-finding phase IIb study evaluated the efficacy and safety of trabedersen (AP 12009) administered intratumorally by convection-enhanced delivery compared with standard chemotherapy in patients with recurrent/refractory high-grade glioma. One hundred and forty-five patients with central reference histopathology of recurrent/refractory glioblastoma multiforme (GBM) or anaplastic astrocytoma (AA) were randomly assigned to receive trabedersen at doses of 10 or 80 µM or standard chemotherapy (temozolomide or procarbazine/lomustine/vincristine). Primary endpoint was 6-month tumor control rate, and secondary endpoints included response at further timepoints, survival, and safety. Six-month tumor control rates were not significantly different in the entire study population (AA and GBM). Prespecified AA subgroup analysis showed a significant benefit regarding the 14-month tumor control rate for 10 µM trabedersen vs chemotherapy (p= .0032). The 2-year survival rate had a trend for superiority for 10 µM trabedersen vs chemotherapy (p = .10). Median survival for 10 µM trabedersen was 39.1 months compared with 35.2 months for 80 µM trabedersen and 21.7 months for chemotherapy (not significant). In GBM patients, response and survival results were comparable among the 3 arms. Exploratory analysis on GBM patients aged ≤55 years with Karnofsky performance status >80% at baseline indicated a 3-fold survival at 2 and 3 years for 10 µM trabedersen vs chemotherapy. The frequency of patients with related or possibly drug-related adverse events was higher with standard chemotherapy (64%) than with 80 µM trabedersen (43%) and 10 µM trabedersen (27%). Superior efficacy and safety for 10 µM trabedersen over 80 µM trabedersen and chemotherapy and positive risk-benefit assessment suggest it as the optimal dose for further clinical development in high-grade glioma.
Figures
Comment in
-
Convection-enhanced delivery of a transforming growth factor-beta2 inhibitor trabedersen for recurrent high-grade gliomas: efficacy real or imagined?, in reference to Bogdahn et al. (Neuro-Oncology 2011;13:132-142).Neuro Oncol. 2011 May;13(5):558-9; author reply 561-2. doi: 10.1093/neuonc/nor048. Neuro Oncol. 2011. PMID: 21558078 Free PMC article. No abstract available.
-
Trabedersen to target transforming growth factor-beta: when the journey is not the reward, in reference to Bogdahn et al. (Neuro-Oncology 2011;13:132-142).Neuro Oncol. 2011 May;13(5):559-60; author reply 561-2. doi: 10.1093/neuonc/nor046. Neuro Oncol. 2011. PMID: 21558079 Free PMC article. No abstract available.
Similar articles
-
Treatment of malignant gliomas with TGF-beta2 antisense oligonucleotides.Expert Rev Anticancer Ther. 2009 Nov;9(11):1663-74. doi: 10.1586/era.09.138. Expert Rev Anticancer Ther. 2009. PMID: 19895249 Review.
-
Trabedersen, a TGFbeta2-specific antisense oligonucleotide for the treatment of malignant gliomas and other tumors overexpressing TGFbeta2.IDrugs. 2009 Jul;12(7):445-53. IDrugs. 2009. PMID: 19579166
-
Convection-enhanced delivery of a transforming growth factor-beta2 inhibitor trabedersen for recurrent high-grade gliomas: efficacy real or imagined?, in reference to Bogdahn et al. (Neuro-Oncology 2011;13:132-142).Neuro Oncol. 2011 May;13(5):558-9; author reply 561-2. doi: 10.1093/neuonc/nor048. Neuro Oncol. 2011. PMID: 21558078 Free PMC article. No abstract available.
-
TGF-β2 signaling in high-grade gliomas.Curr Pharm Biotechnol. 2011 Dec;12(12):2150-7. doi: 10.2174/138920111798808347. Curr Pharm Biotechnol. 2011. PMID: 21619538 Review.
-
The antisense oligonucleotide trabedersen (AP 12009) for the targeted inhibition of TGF-β2.Curr Pharm Biotechnol. 2011 Dec;12(12):2203-13. doi: 10.2174/138920111798808266. Curr Pharm Biotechnol. 2011. PMID: 21619536 Review.
Cited by
-
Snail depletes the tumorigenic potential of glioblastoma.Oncogene. 2013 Nov 21;32(47):5409-20. doi: 10.1038/onc.2013.67. Epub 2013 Mar 25. Oncogene. 2013. PMID: 23524585 Free PMC article.
-
Strategies to use immune modulators in therapeutic vaccines against cancer.Semin Oncol. 2012 Jun;39(3):348-57. doi: 10.1053/j.seminoncol.2012.02.002. Semin Oncol. 2012. PMID: 22595057 Free PMC article. Review.
-
An antisense oligonucleotide against SOD1 delivered intrathecally for patients with SOD1 familial amyotrophic lateral sclerosis: a phase 1, randomised, first-in-man study.Lancet Neurol. 2013 May;12(5):435-42. doi: 10.1016/S1474-4422(13)70061-9. Epub 2013 Mar 29. Lancet Neurol. 2013. PMID: 23541756 Free PMC article. Clinical Trial.
-
Transforming growth factor-β pathway activity in glioblastoma.Oncotarget. 2015 Mar 20;6(8):5963-77. doi: 10.18632/oncotarget.3467. Oncotarget. 2015. PMID: 25849941 Free PMC article.
-
Recent Advances in Oligonucleotide Therapeutics in Oncology.Int J Mol Sci. 2021 Mar 24;22(7):3295. doi: 10.3390/ijms22073295. Int J Mol Sci. 2021. PMID: 33804856 Free PMC article. Review.
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–996. doi:10.1056/NEJMoa043330. - DOI - PubMed
-
- Stupp R, Hegi ME, Mason WP, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–466. doi:10.1016/S1470-2045(09)70025-7. - DOI - PubMed
-
- Chang SM, Theodosopoulos P, Lamborn K, et al. Temozolomide in the treatment of recurrent malignant glioma. Cancer. 2004;100:605–611. doi:10.1002/cncr.11949. - DOI - PubMed
-
- Fontana A, Bodmer S, Frei K, Malipiero U, Siepl C. Expression of TGF-beta2 in human glioblastoma: a role in resistance to immune rejection? CIBA Found Symp. 1991;157:232–241. - PubMed
-
- Maxwell M, Galanopoulos T, Neville-Golden J, Antoniades HN. Effect of the expression of transforming growth factor-beta 2 in primary human glioblastomas on immunosuppression and loss of immune surveillance. J Neurosurg. 1992;76:799–804. doi:10.3171/jns.1992.76.5.0799. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
