

Impact of scar burden by single-photon emission computed tomography myocardial perfusion imaging on patient outcomes following cardiac resynchronization therapy
- PMID: 20971745
- PMCID: PMC3013201
- DOI: 10.1093/eurheartj/ehq389
Impact of scar burden by single-photon emission computed tomography myocardial perfusion imaging on patient outcomes following cardiac resynchronization therapy
Abstract
Aims: Ischaemic heart disease negatively impacts response to cardiac resynchronization therapy (CRT), yet the impact of infarct scar burden on clinical outcomes and its interaction with mechanical dyssynchrony have not been well described.
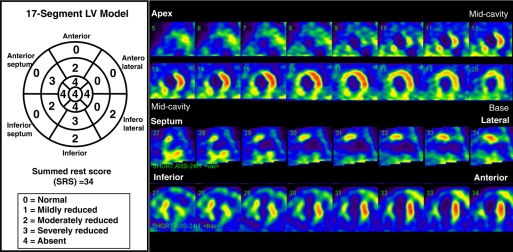
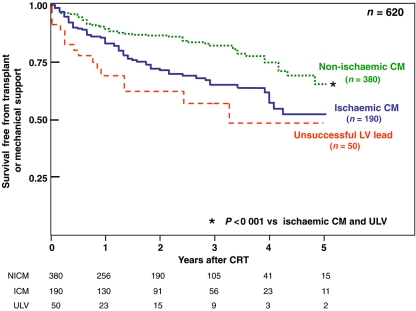
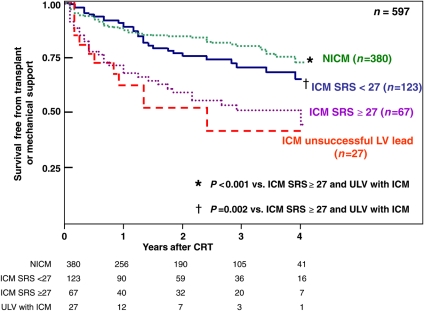
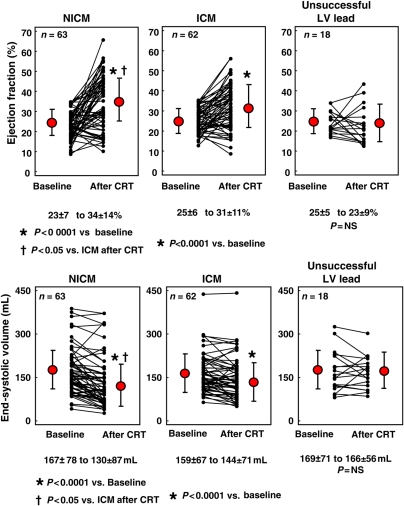
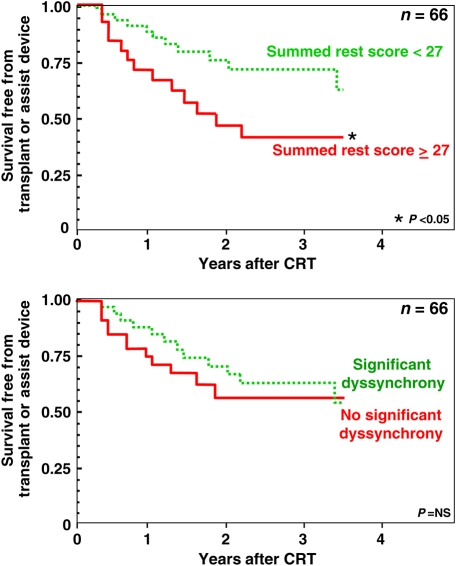
Methods and results: We studied 620 NYHA classes III-IV heart failure patients with ejection fraction (EF) ≤ 35% and QRS duration ≥120 ms referred for CRT. Included were 190 ischaemic cardiomyopathy (ICM) CRT recipients with scar burden quantified by rest-redistribution Tl(201) myocardial perfusion imaging using a 17-segment (0 = normal to 4 = absence of uptake) summed rest score (SRS). Non-ICM (NICM) CRT recipients (n = 380) and 50 patients referred for CRT with unsuccessful LV lead implant comprised the comparison groups. Echocardiographic dyssynchrony analysis was performed in a subgroup of 150 patients. Follow-up left ventricular EF (LVEF) and volumes were examined at 7 ± 3 months in 143 patients. The outcome of death, cardiac transplant, or mechanical circulatory support was assessed in all. Over 2.1 ± 1.6 years, ICM patients had significantly worse survival and less LVEF improvement than NICM patients (P < 0.01). Ischaemic cardiomyopathy patients with low scar burden (SRS < 27) had favourable survival and LVEF improvement, similar to NICM patients. A high scar burden (SRS ≥ 27) was associated with reduced survival and lack of LV functional improvement (P ≤ 0.01), similar to those with unsuccessful LV lead implant, whereas baseline dyssynchrony was not predictive of outcome in these patients.
Conclusion: Extensive scar burden in ICM patients unfavourably affected clinical and LV functional outcomes after CRT, regardless of baseline dyssynchrony measures. Patients with ICM and lower scar burden had significantly better outcomes, similar to NICM patients.
Figures

Similar articles
-
Scar burden, not intraventricular conduction delay pattern, is associated with outcomes in ischemic cardiomyopathy patients receiving cardiac resynchronization therapy.Heart Rhythm. 2018 Nov;15(11):1664-1672. doi: 10.1016/j.hrthm.2018.05.027. Epub 2018 May 28. Heart Rhythm. 2018. PMID: 29852239
-
Cardiac resynchronization therapy and bone marrow cell transplantation in patients with ischemic heart failure and electromechanical dyssynchrony: a randomized pilot study.J Cardiovasc Transl Res. 2011 Dec;4(6):767-78. doi: 10.1007/s12265-011-9283-1. Epub 2011 May 6. J Cardiovasc Transl Res. 2011. PMID: 21547598 Clinical Trial.
-
Scar burden by myocardial perfusion imaging predicts echocardiographic response to cardiac resynchronization therapy in ischemic cardiomyopathy.Am Heart J. 2007 Jan;153(1):105-12. doi: 10.1016/j.ahj.2006.10.015. Am Heart J. 2007. PMID: 17174647
-
Assessment of mechanical dyssynchrony in cardiac resynchronization therapy.Dan Med J. 2014 Dec;61(12):B4981. Dan Med J. 2014. PMID: 25441737 Review.
-
Role of nuclear imaging in cardiac resynchronization therapy.Expert Rev Cardiovasc Ther. 2009 Jan;7(1):65-72. doi: 10.1586/14779072.7.1.65. Expert Rev Cardiovasc Ther. 2009. PMID: 19105768 Review.
Cited by
-
Myocardial viability as integral part of the diagnostic and therapeutic approach to ischemic heart failure.J Nucl Cardiol. 2015 Apr;22(2):229-45. doi: 10.1007/s12350-015-0096-5. Epub 2015 Mar 3. J Nucl Cardiol. 2015. PMID: 25733105 Free PMC article. Review.
-
Cardiac dyssynchrony: we have the tools. It is time to use them.J Nucl Cardiol. 2012 Jun;19(3):420-3. doi: 10.1007/s12350-012-9526-9. J Nucl Cardiol. 2012. PMID: 22362266 No abstract available.
-
Biventricular Pacing Going Along with Acute Hemodynamic Response in a Patient with Huge Anterior Wall Aneurysm - Importance of Pacing Viable Myocardium.Am J Case Rep. 2019 Jun 9;20:810-815. doi: 10.12659/AJCR.914480. Am J Case Rep. 2019. PMID: 31177265 Free PMC article.
-
The Value of Left Ventricular Mechanical Dyssynchrony and Scar Burden in the Combined Assessment of Factors Associated with Cardiac Resynchronization Therapy Response in Patients with CRT-D.J Clin Med. 2023 Mar 8;12(6):2120. doi: 10.3390/jcm12062120. J Clin Med. 2023. PMID: 36983123 Free PMC article.
-
The relationship of QRS morphology and mechanical dyssynchrony to long-term outcome following cardiac resynchronization therapy.Eur Heart J. 2012 Nov;33(21):2680-91. doi: 10.1093/eurheartj/ehs013. Epub 2012 Feb 19. Eur Heart J. 2012. PMID: 22351700 Free PMC article.
References
-
- Abraham WT, Fisher WG, Smith AL, Delurgio DB, Leon AR, Loh E, Kocovic DZ, Packer M, Clavell AL, Hayes DL, Ellestad M, Trupp RJ, Underwood J, Pickering F, Truex C, McAtee P, Messenger J. Cardiac resynchronization in chronic heart failure. N Engl J Med. 2002;346:1845–1853. - PubMed
-
- Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass DA, De Marco T, Carson P, DiCarlo L, DeMets D, White BG, DeVries DW, Feldman AM. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350:2140–2150. - PubMed
-
- Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L, Tavazzi L. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352:1539–1549. - PubMed
-
- Bax JJ, Bleeker GB, Marwick TH, Molhoek SG, Boersma E, Steendijk P, van der Wall EE, Schalij MJ. Left ventricular dyssynchrony predicts response and prognosis after cardiac resynchronization therapy. J Am Coll Cardiol. 2004;44:1834–1840. - PubMed
-
- Bax JJ, Abraham T, Barold SS, Breithardt OA, Fung JW, Garrigue S, Gorcsan J, III, Hayes DL, Kass DA, Knuuti J, Leclercq C, Linde C, Mark DB, Monaghan MJ, Nihoyannopoulos P, Schalij MJ, Stellbrink C, Yu CM. Cardiac resynchronization therapy: Part 1—issues before device implantation. J Am Coll Cardiol. 2005;46:2153–2167. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
