

CMV in critically ill patients: pathogen or bystander?
- PMID: 20931610
- PMCID: PMC2987685
- DOI: 10.1002/rmv.664
CMV in critically ill patients: pathogen or bystander?
Abstract
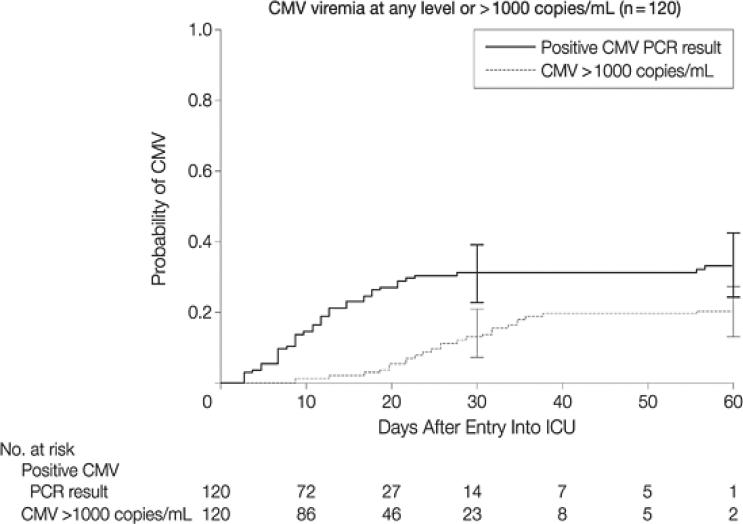
Despite broad variability in study populations, methodologies for CMV detection, and analytic methods used, multiple studies have documented frequent CMV infection in non-immunocompromised adults with critical illness due to a variety of causes. Higher rates of CMV infection in studies of seropositive patients suggest that reactivation of latent infection rather than primary infection is the main mechanism in this setting. Risk factors for CMV reactivation (other than seropositivity) have not been clearly defined and there does not appear to be a consistent association with severity of illness. Furthermore, CMV reactivation in this setting has been associated with important adverse clinical outcomes, including increased duration of mechanical ventilation, longer length of stay and all-cause mortality. There are several biologically plausible mechanisms that could link CMV reactivation with adverse outcomes, including: direct lung injury (CMV pneumonia), amplification of inflammation systemically and within the lung, or predisposition to other nosocomial infections, but clinical data in the ICU setting are limited. Further observational studies are unlikely to significantly advance our understanding of the role of CMV in critically ill patients. Given the significant impact of critical illness, limited current therapeutic options, the availability of generally well-tolerated antiviral options for CMV, and the clinical data supporting a possible pathogenic role for CMV, there is a strong rationale for a randomised controlled trial of CMV prevention as a novel means of improving the outcomes of critically ill patients.
2010 John Wiley & Sons, Ltd.
Figures
Similar articles
-
Cytomegalovirus reactivation in critically ill immunocompetent patients.JAMA. 2008 Jul 23;300(4):413-22. doi: 10.1001/jama.300.4.413. JAMA. 2008. PMID: 18647984 Free PMC article.
-
Cytomegalovirus reactivation in a general, nonimmunosuppressed intensive care unit population: incidence, risk factors, associations with organ dysfunction, and inflammatory biomarkers.J Crit Care. 2015 Apr;30(2):276-81. doi: 10.1016/j.jcrc.2014.10.002. Epub 2014 Oct 8. J Crit Care. 2015. PMID: 25457114
-
Effect of Ganciclovir on IL-6 Levels Among Cytomegalovirus-Seropositive Adults With Critical Illness: A Randomized Clinical Trial.JAMA. 2017 Aug 22;318(8):731-740. doi: 10.1001/jama.2017.10569. JAMA. 2017. PMID: 28829877 Free PMC article. Clinical Trial.
-
Cytomegalovirus infection in non-immunosuppressed critically ill patients.J Infect Dev Ctries. 2011 Aug 12;5(8):571-9. doi: 10.3855/jidc.1487. J Infect Dev Ctries. 2011. PMID: 21841300 Review.
-
[Citomegalovirus reactivation in critical ill intensive care patients].Gac Med Mex. 2011 Mar-Apr;147(2):159-62. Gac Med Mex. 2011. PMID: 21527972 Review. Spanish.
Cited by
-
Metagenomic next-generation sequencing for mixed pulmonary infection diagnosis.BMC Pulm Med. 2019 Dec 19;19(1):252. doi: 10.1186/s12890-019-1022-4. BMC Pulm Med. 2019. PMID: 31856779 Free PMC article.
-
Herpes DNAemia and TTV Viraemia in Intensive Care Unit Critically Ill Patients: A Single-Centre Prospective Longitudinal Study.Front Immunol. 2021 Nov 2;12:698808. doi: 10.3389/fimmu.2021.698808. eCollection 2021. Front Immunol. 2021. PMID: 34795661 Free PMC article.
-
Cytomegalovirus reactivation in a critically ill patient: a case report.J Med Case Rep. 2018 Jun 11;12(1):163. doi: 10.1186/s13256-018-1681-4. J Med Case Rep. 2018. PMID: 29886847 Free PMC article.
-
The diagnostic value of metagenomics next-generation sequencing in HIV-infected patients with suspected pulmonary infections.Front Cell Infect Microbiol. 2024 May 7;14:1395239. doi: 10.3389/fcimb.2024.1395239. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 38774626 Free PMC article.
-
Update in Viral Infections in the Intensive Care Unit.Front Med (Lausanne). 2021 Feb 23;8:575580. doi: 10.3389/fmed.2021.575580. eCollection 2021. Front Med (Lausanne). 2021. PMID: 33708775 Free PMC article. Review.
References
-
- Kalil AC, Florescu DF. Prevalence and mortality associated with cytomegalovirus infection in nonimmunosuppressed patients in the intensive care unit. Crit Care Med. 2009 Aug;37(8):2350–2358. - PubMed
-
- Hamprecht K, Baumeister A, Beck R, Haeberle H, Heininger A. The lung as a central compartment of active CMV infection. Inflammation Research Supplement 2. 2007:S242. (Abstract A383)
-
- Domart Y, Trouillet JL, Fagon JY, Chastre J, Brun-Vezinet F, Gibert C. Incidence and morbidity of cytomegaloviral infection in patients with mediastinitis following cardiac surgery. Chest. 1990 Jan;97(1):18–22. - PubMed
-
- Papazian L, Fraisse A, Garbe L, et al. Cytomegalovirus. An unexpected cause of ventilator-associated pneumonia. Anesthesiology. 1996 Feb;84(2):280–287. - PubMed
