

Low temperature of radiofrequency ablation at the target sites can facilitate rapid progression of residual hepatic VX2 carcinoma
- PMID: 20667141
- PMCID: PMC2917410
- DOI: 10.1186/1479-5876-8-73
Low temperature of radiofrequency ablation at the target sites can facilitate rapid progression of residual hepatic VX2 carcinoma
Abstract
Background: Rapid progression of residual tumor after radiofrequency ablation (RFA) of hepatocellular carcinoma has been observed increasingly. However, its underlying mechanisms remain to be clarified. The present study was designed to determine whether low temperature of RFA at the target sites facilitates rapid progression of residual hepatic VX2 carcinoma and to clarify the possible underlying mechanisms.
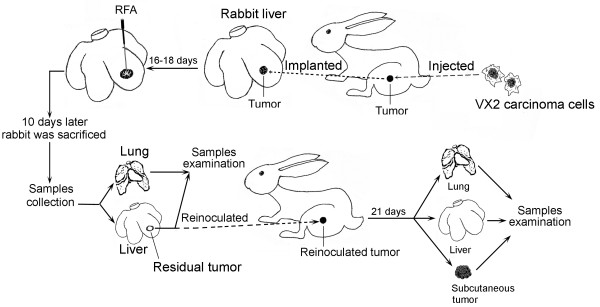
Methods: The residual VX2 hepatoma model in rabbits was established by using RFA at 55, 70 and 85 degrees C. Rabbits that were implanted with VX2 hepatoma but did not receive RFA acted as a control group. The relationship between rapid progression of residual hepatic VX2 carcinoma and low temperature of RFA at the target sites was carefully evaluated. A number of potential contributing molecular factors, such as proliferating cell nuclear antigen (PCNA), matrix metalloproteinase 9 (MMP-9), vascular endothelial growth factor (VEGF), hepatocyte growth factor (HGF) and Interleukin-6 (IL-6) were measured.
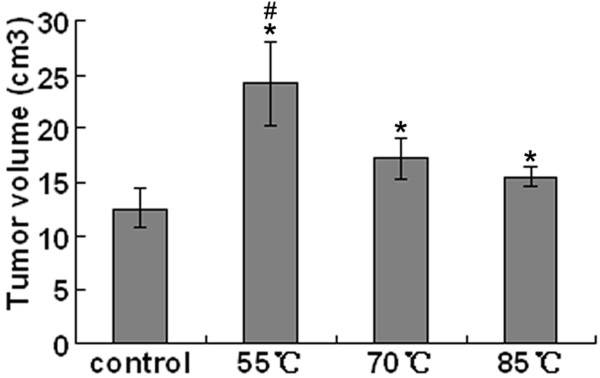
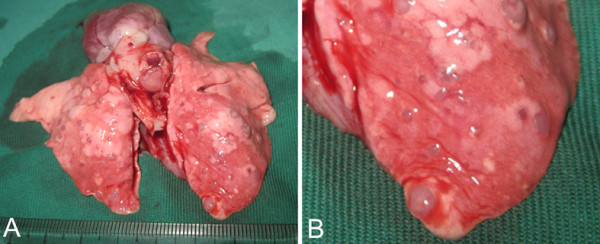
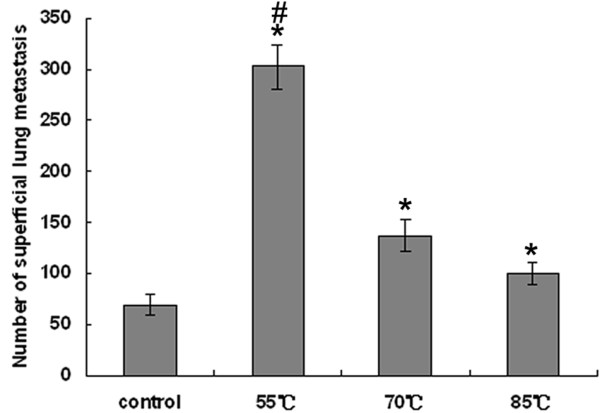
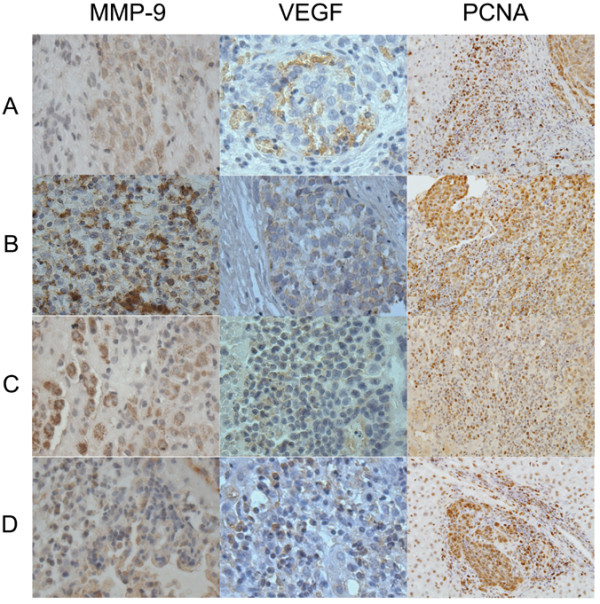
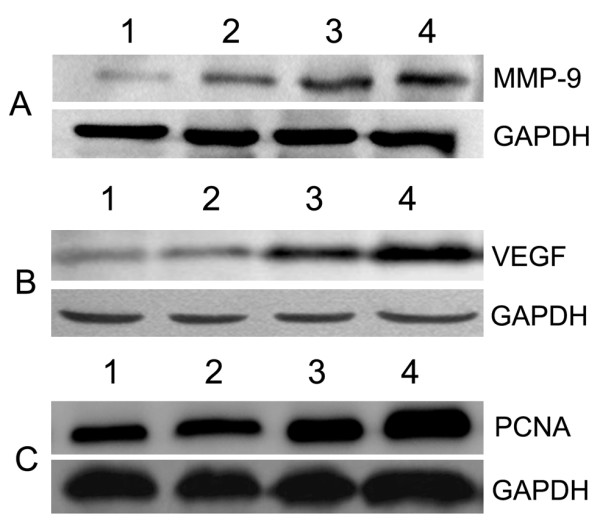
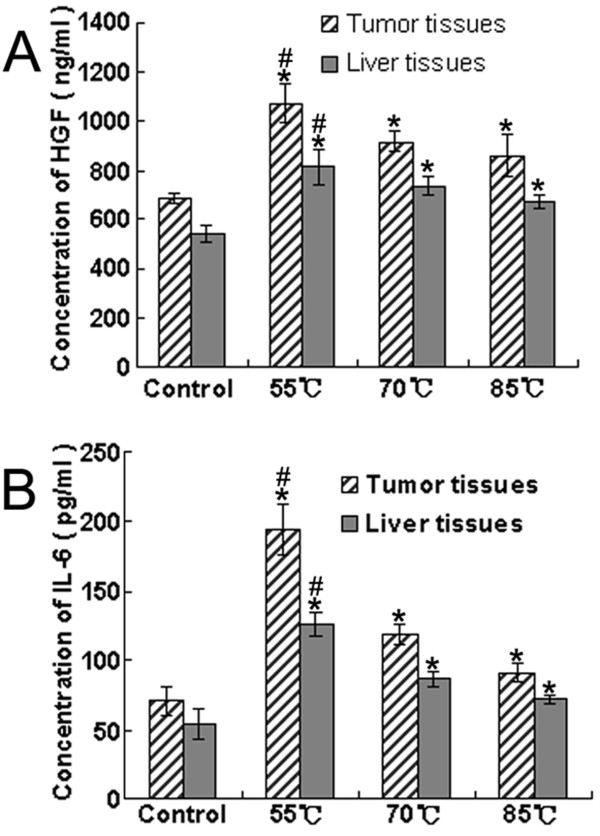
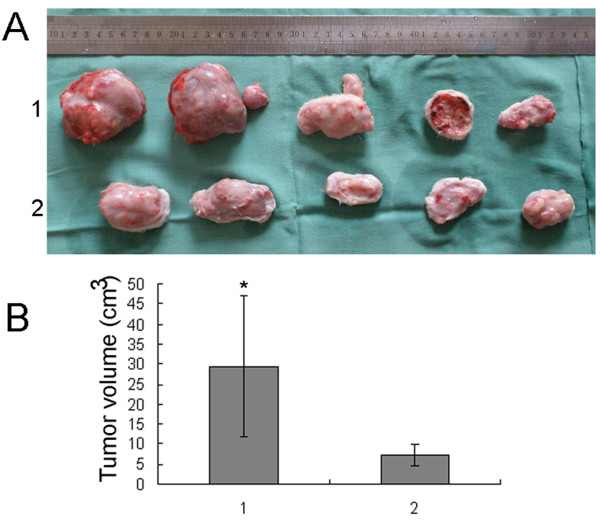
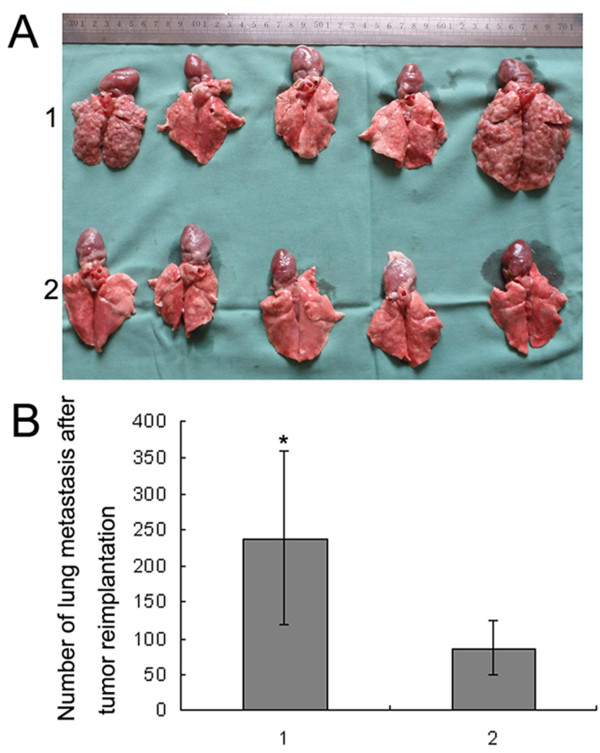
Results: The focal tumor volume and lung metastases of RFA-treated rabbits increased significantly compared with the control group (P < 0.05), and the greatest changes were seen in the 55 degrees C group (P < 0.05). Expression of PCNA, MMP-9, VEGF, HGF and IL-6 in tumor tissues increased significantly in the RFA-treated groups compared with the control group, and of the increases were greatest in the 55 degrees C group (P < 0.05). These results were consistent with gross pathological observation. Tumor re-inoculation experiments confirmed that low temperature of RFA at the target sites facilitated rapid progression of residual hepatic VX2 carcinoma.
Conclusions: Insufficient RFA that is caused by low temperature at the target sites could be an important cause of rapid progression of residual hepatic VX2 carcinoma. Residual hepatic VX2 carcinoma could facilitate its rapid progression through inducing overexpression of several molecular factors, such as PCNA, MMP-9, VEGF, HGF and IL-6.
Figures
Similar articles
-
Inflammation and cancer: inhibiting the progression of residual hepatic VX2 carcinoma by anti-inflammatory drug after incomplete radiofrequency ablation.Int J Clin Exp Pathol. 2015 Nov 1;8(11):13945-56. eCollection 2015. Int J Clin Exp Pathol. 2015. PMID: 26823706 Free PMC article.
-
Angiogenesis in residual cancer and roles of HIF-1α, VEGF, and MMP-9 in the development of residual cancer after radiofrequency ablation and surgical resection in rabbits with liver cancer.Folia Morphol (Warsz). 2020;79(1):71-78. doi: 10.5603/FM.a2019.0059. Epub 2019 May 20. Folia Morphol (Warsz). 2020. PMID: 31106843
-
No-Touch Radiofrequency Ablation of VX2 Hepatic Tumors In Vivo in Rabbits: A Proof of Concept Study.Korean J Radiol. 2018 Nov-Dec;19(6):1099-1109. doi: 10.3348/kjr.2018.19.6.1099. Epub 2018 Oct 18. Korean J Radiol. 2018. PMID: 30386141 Free PMC article.
-
Radiofrequency (thermal) ablation versus no intervention or other interventions for hepatocellular carcinoma.Cochrane Database Syst Rev. 2013 Dec 19;(12):CD003046. doi: 10.1002/14651858.CD003046.pub3. Cochrane Database Syst Rev. 2013. PMID: 24357457 Review.
-
An Overview of Hepatocellular Carcinoma After Insufficient Radiofrequency Ablation.J Hepatocell Carcinoma. 2022 Apr 26;9:343-355. doi: 10.2147/JHC.S358539. eCollection 2022. J Hepatocell Carcinoma. 2022. PMID: 35502292 Free PMC article. Review.
Cited by
-
Mechanisms and therapeutic strategies to combat the recurrence and progression of hepatocellular carcinoma after thermal ablation.J Interv Med. 2023 Oct 18;6(4):160-169. doi: 10.1016/j.jimed.2023.10.004. eCollection 2023 Nov. J Interv Med. 2023. PMID: 38312128 Free PMC article.
-
Sub-lethal hyperthermia promotes epithelial-to-mesenchymal-like transition of breast cancer cells: implication of the synergy between hyperthermia and chemotherapy.RSC Adv. 2018 Dec 20;9(1):52-57. doi: 10.1039/c8ra08472f. eCollection 2018 Dec 19. RSC Adv. 2018. PMID: 35521586 Free PMC article.
-
Does Radiofrequency Ablation Induce Neoplastic Changes in Benign Thyroid Nodules: A Preliminary Study.Endocrinol Metab (Seoul). 2019 Jun;34(2):169-178. doi: 10.3803/EnM.2019.34.2.169. Epub 2019 May 15. Endocrinol Metab (Seoul). 2019. PMID: 31099203 Free PMC article.
-
Heat treatment-induced autophagy promotes breast cancer cell invasion and metastasis via TGF-β2-mediated epithelial-mesenchymal transitions.PeerJ. 2023 Jan 12;11:e14640. doi: 10.7717/peerj.14640. eCollection 2023. PeerJ. 2023. PMID: 36650834 Free PMC article.
-
Molecular targeting agents associated with transarterial chemoembolization or radiofrequency ablation in hepatocarcinoma treatment.World J Gastroenterol. 2014 Jan 14;20(2):486-97. doi: 10.3748/wjg.v20.i2.486. World J Gastroenterol. 2014. PMID: 24574717 Free PMC article. Review.
References
-
- Sun WB. How is radiofrequency ablation going in treating hepatocellular carcinoma in China? Austral-Asian Journal of Cancer. 2008;7(4):221–224.
-
- Thanos L, Mylona S, Galani P, Pomoni M, Pomoni A, Koskinas I. Overcoming the heat-sink phenomenon: successful radiofrequency thermal ablation of liver tumors in contact with blood vessels. Diagn Interv Radiol. 2008;14(1):51–56. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
