

Dichotomy in duration and severity of acute inflammatory responses in humans arising from differentially expressed proresolution pathways
- PMID: 20421472
- PMCID: PMC2889345
- DOI: 10.1073/pnas.1000373107
Dichotomy in duration and severity of acute inflammatory responses in humans arising from differentially expressed proresolution pathways
Abstract
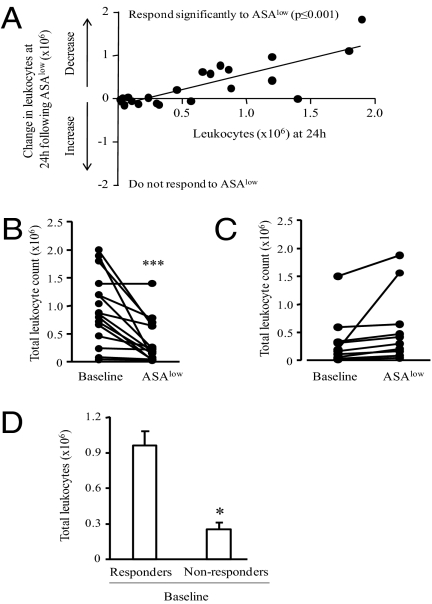
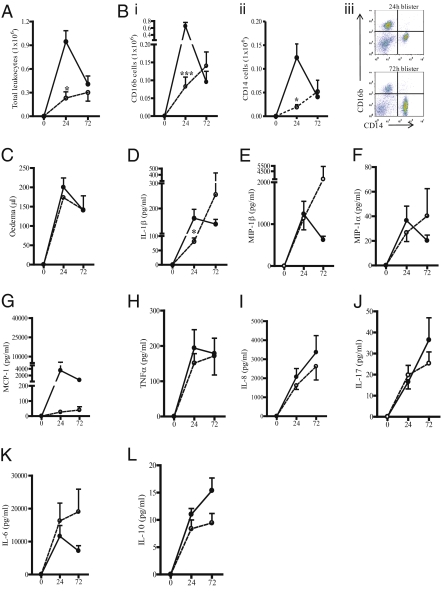
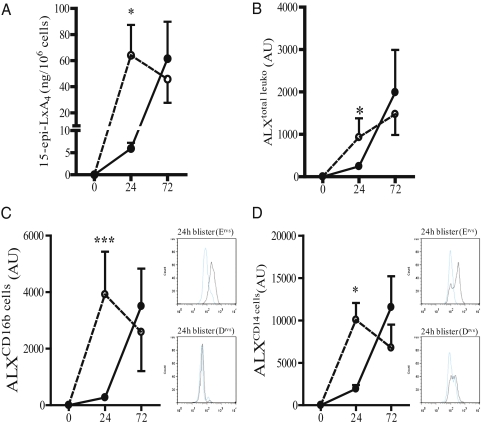
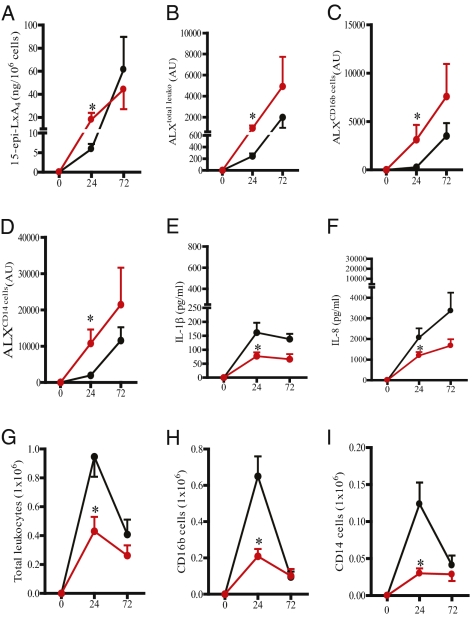
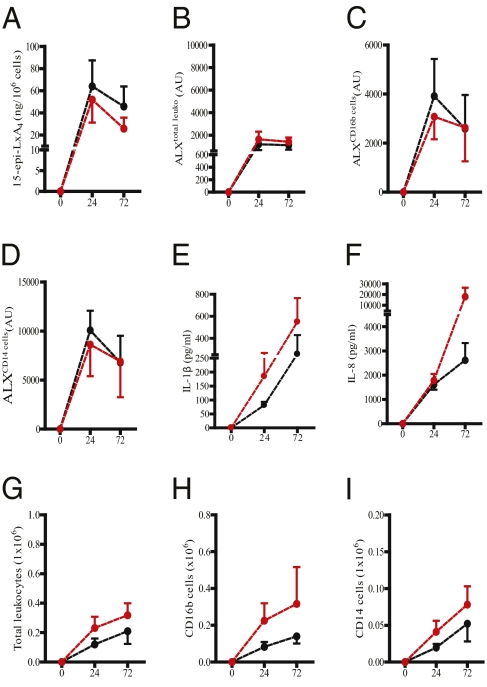
Lipoxins (Lxs) and aspirin-triggered epi-Lxs (15-epi-LxA(4)) act through the ALX/FPRL1 receptor to block leukocyte trafficking, dampen cytokine/chemokine synthesis, and enhance phagocytic clearance of apoptotic leukocytes-key requisites for inflammatory resolution. Although studies using primarily inbred rodents have highlighted resolution as an active event, little is known about the role resolution pathways play in controlling the duration/profile of inflammatory responses in humans. To examine this, we found two types of responders to cantharidin-induced skin blisters in male healthy volunteers: those with immediate leukocyte accumulation and cytokine/chemokine synthesis followed by early resolution and a second group whose inflammation increased gradually over time followed by delayed resolution. In early resolvers, blister 15-epi-LxA(4) and leukocyte ALX were low, but increased as inflammation abated. In contrast, in delayed resolvers, 15-epi-LxA(4) and ALX were high early in the response but waned as inflammation progressed. Elevating 15-epi-LxA(4) in early resolvers using aspirin increased blister leukocyte ALX but reduced cytokines/chemokines as well as polymorphonuclear leukocyte and macrophage numbers. These findings show that two phenotypes exist in humans with respect to inflammation severity/longevity controlled by proresolution mediators, namely 15-epi-LxA(4). These data have implications for understanding the etiology of chronic inflammation and future directions in antiinflammatory therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Effects of low-dose aspirin on acute inflammatory responses in humans.J Immunol. 2009 Aug 1;183(3):2089-96. doi: 10.4049/jimmunol.0900477. Epub 2009 Jul 13. J Immunol. 2009. PMID: 19597002 Clinical Trial.
-
Selectivity of recombinant human leukotriene D(4), leukotriene B(4), and lipoxin A(4) receptors with aspirin-triggered 15-epi-LXA(4) and regulation of vascular and inflammatory responses.Am J Pathol. 2001 Jan;158(1):3-9. doi: 10.1016/S0002-9440(10)63937-5. Am J Pathol. 2001. PMID: 11141472 Free PMC article.
-
Lipoxin A4 and aspirin-triggered 15-epi-lipoxin A4 inhibit human neutrophil migration: comparisons between synthetic 15 epimers in chemotaxis and transmigration with microvessel endothelial cells and epithelial cells.J Immunol. 2003 Mar 1;170(5):2688-94. doi: 10.4049/jimmunol.170.5.2688. J Immunol. 2003. PMID: 12594298
-
The lipoxin receptor ALX: potent ligand-specific and stereoselective actions in vivo.Pharmacol Rev. 2006 Sep;58(3):463-87. doi: 10.1124/pr.58.3.4. Pharmacol Rev. 2006. PMID: 16968948 Review.
-
Lipid-derived mediators in endogenous anti-inflammation and resolution: lipoxins and aspirin-triggered 15-epi-lipoxins.ScientificWorldJournal. 2002 Jan 22;2:169-204. doi: 10.1100/tsw.2002.81. ScientificWorldJournal. 2002. PMID: 12806051 Free PMC article. Review.
Cited by
-
Aspirin triggered-lipoxin A4 reduces the adhesion of human polymorphonuclear neutrophils to endothelial cells initiated by preeclamptic plasma.Prostaglandins Leukot Essent Fatty Acids. 2012 Oct-Nov;87(4-5):127-34. doi: 10.1016/j.plefa.2012.08.003. Epub 2012 Sep 10. Prostaglandins Leukot Essent Fatty Acids. 2012. PMID: 22974760 Free PMC article.
-
Pathway Markers for Pro-resolving Lipid Mediators in Maternal and Umbilical Cord Blood: A Secondary Analysis of the Mothers, Omega-3, and Mental Health Study.Front Pharmacol. 2016 Sep 7;7:274. doi: 10.3389/fphar.2016.00274. eCollection 2016. Front Pharmacol. 2016. PMID: 27656142 Free PMC article.
-
Lipid mediators in immune regulation and resolution.Br J Pharmacol. 2019 Apr;176(8):1009-1023. doi: 10.1111/bph.14587. Epub 2019 Mar 1. Br J Pharmacol. 2019. PMID: 30674066 Free PMC article. Review.
-
Resolution of acute inflammation in the lung.Annu Rev Physiol. 2014;76:467-92. doi: 10.1146/annurev-physiol-021113-170408. Epub 2013 Dec 2. Annu Rev Physiol. 2014. PMID: 24313723 Free PMC article. Review.
-
Pro-resolving lipid mediators are leads for resolution physiology.Nature. 2014 Jun 5;510(7503):92-101. doi: 10.1038/nature13479. Nature. 2014. PMID: 24899309 Free PMC article. Review.
References
-
- Gilroy DW, Lawrence T, Perretti M, Rossi AG. Inflammatory resolution: New opportunities for drug discovery. Nat Rev Drug Discov. 2004;3:401–416. - PubMed
-
- Hallett JM, et al. Novel pharmacological strategies for driving inflammatory cell apoptosis and enhancing the resolution of inflammation. Trends Pharmacol Sci. 2008;29:250–257. - PubMed
-
- Serhan CN, Savill J. Resolution of inflammation: The beginning programs the end. Nat Immunol. 2005;6:1191–1197. - PubMed
-
- Serhan CN. Lipoxins and aspirin-triggered 15-epi-lipoxin biosynthesis: An update and role in anti-inflammation and pro-resolution. Prostaglandins Other Lipid Mediat. 2002;68-69:433–455. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
