

Persistence of cognitive impairment after resolution of overt hepatic encephalopathy
- PMID: 20178797
- PMCID: PMC2883684
- DOI: 10.1053/j.gastro.2010.02.015
Persistence of cognitive impairment after resolution of overt hepatic encephalopathy
Abstract
Background & aims: In patients with cirrhosis, hepatic encephalopathy (HE) has acute but reversible as well as chronic components. We investigated the extent of residual cognitive impairment following clinical resolution of overt HE (OHE).
Methods: Cognitive function of cirrhotic patients was evaluated using psychometric tests (digit symbol, block design, and number connection [NCT-A and B]) and the inhibitory control test (ICT). Improvement (reduction) in ICT lures and first minus second halves (DeltaL(1-2)) were used to determine learning of response inhibition. Two cross-sectional studies (A and B) compared data from stable cirrhotic patients with or without prior OHE. We then prospectively assessed cognitive performance, before and after the first episode of OHE.
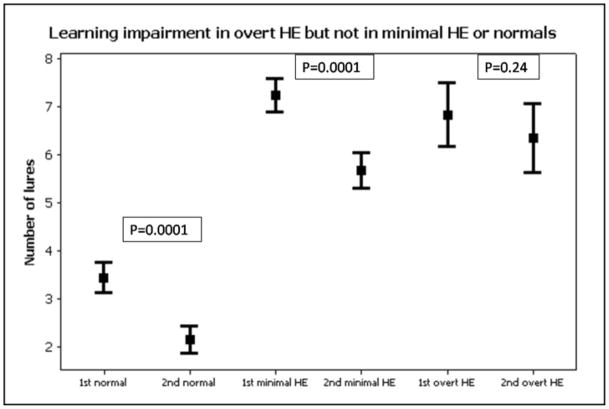
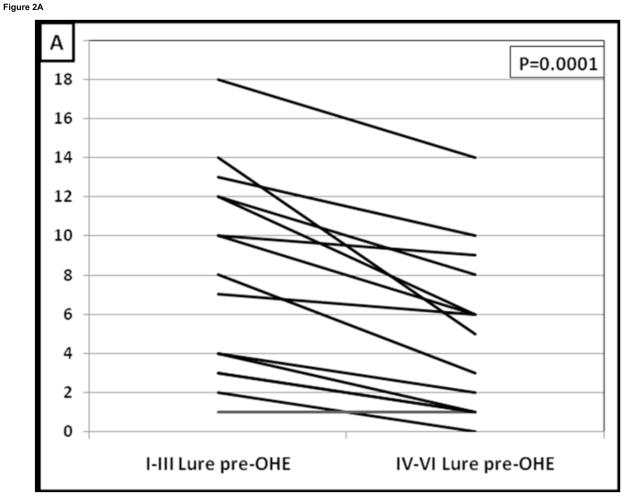
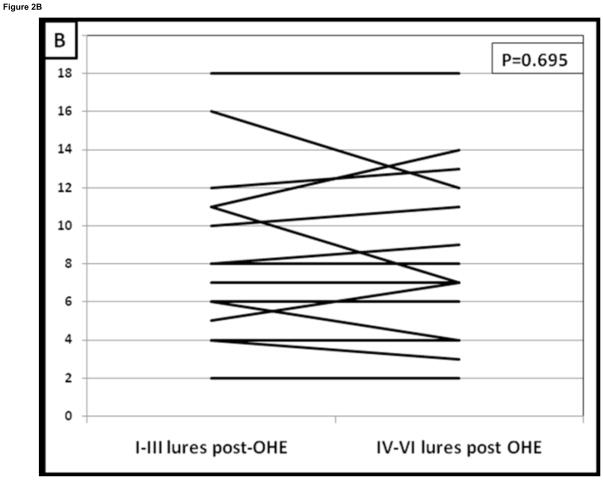
Results: In study A (226 cirrhotic patients), 54 had experienced OHE, 120 had minimal HE, and 52 with no minimal HE. Despite normal mental status on lactulose after OHE, cirrhotic patients were cognitively impaired, based on results from all tests. Learning of response inhibition (DeltaL(1-2) > or =1) was evident in patients with minimal HE and no minimal HE but was lost after OHE. In study B (50 additional patients who developed > or =1 documented OHE episode during follow-up), the number of OHE hospitalizations correlated with severity of residual impairment, indicated by ICT lures (r = 0.5, P = .0001), digit symbol test (r = -0.39, P = .002), and number connection test-B (r = 0.33, P = .04). In the prospective study (59 cirrhotic patients without OHE), 15 developed OHE; ICT lure response worsened significantly after OHE (12 before vs 18 after, P = .0003), and learning of response inhibition was lost. The 44 patients who did not experience OHE did not have deteriorations in cognitive function in serial testing.
Conclusions: In cirrhosis, episodes of OHE are associated with persistent and cumulative deficits in working memory, response inhibition, and learning.
Copyright 2010 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Persistence of cognitive impairment after resolution of overt hepatic encephalopathy.Am J Gastroenterol. 2014 Jul;109(7):1011-9. doi: 10.1038/ajg.2014.107. Epub 2014 Apr 29. Am J Gastroenterol. 2014. PMID: 24777152
-
Overt hepatic encephalopathy impairs learning on the EncephalApp stroop which is reversible after liver transplantation.Liver Transpl. 2017 Nov;23(11):1396-1403. doi: 10.1002/lt.24864. Liver Transpl. 2017. PMID: 28885772 Free PMC article.
-
Increased risk of cognitive impairment in cirrhotic patients with bacterial infections.J Hepatol. 2013 Aug;59(2):243-50. doi: 10.1016/j.jhep.2013.03.012. Epub 2013 Mar 21. J Hepatol. 2013. PMID: 23523580
-
Clinical and Neurologic Manifestation of Minimal Hepatic Encephalopathy and Overt Hepatic Encephalopathy.Clin Liver Dis. 2015 Aug;19(3):461-72. doi: 10.1016/j.cld.2015.05.003. Clin Liver Dis. 2015. PMID: 26195201 Review.
-
Prediction and prevention of the first episode of overt hepatic encephalopathy in patients with cirrhosis.Hepatol Commun. 2023 Mar 17;7(4):e0096. doi: 10.1097/HC9.0000000000000096. eCollection 2023 Apr 1. Hepatol Commun. 2023. PMID: 36930868 Free PMC article. Review.
Cited by
-
Hepatic Encephalopathy and Astrocyte Senescence.J Clin Exp Hepatol. 2018 Sep;8(3):294-300. doi: 10.1016/j.jceh.2018.05.003. Epub 2018 May 18. J Clin Exp Hepatol. 2018. PMID: 30302047 Free PMC article. Review.
-
Hepatic encephalopathy.Nat Rev Dis Primers. 2022 Jun 23;8(1):43. doi: 10.1038/s41572-022-00366-6. Nat Rev Dis Primers. 2022. PMID: 35739133 Review.
-
Management of Hepatic Encephalopathy Not Responsive to First-Line Treatments.Curr Treat Options Gastroenterol. 2018 Jun;16(2):253-259. doi: 10.1007/s11938-018-0183-1. Curr Treat Options Gastroenterol. 2018. PMID: 29705917 Review.
-
Fecal microbiota transplant from a rational stool donor improves hepatic encephalopathy: A randomized clinical trial.Hepatology. 2017 Dec;66(6):1727-1738. doi: 10.1002/hep.29306. Epub 2017 Oct 30. Hepatology. 2017. PMID: 28586116 Free PMC article. Clinical Trial.
-
Improving Medication-Related Outcomes in Chronic Liver Disease.Hepatol Commun. 2020 Oct 10;4(11):1562-1577. doi: 10.1002/hep4.1612. eCollection 2020 Nov. Hepatol Commun. 2020. PMID: 33163829 Free PMC article. Review.
References
-
- Bajaj JS, Wade JB, Sanyal AJ. Spectrum of neurocognitive impairment in cirrhosis: Implications for the assessment of hepatic encephalopathy. Hepatology. 2009;50:2014–21. - PubMed
-
- Ortiz M, Jacas C, Cordoba J. Minimal hepatic encephalopathy: diagnosis, clinical significance and recommendations. J Hepatol. 2005;42 (Suppl):S45–53. - PubMed
-
- Prasad S, Dhiman RK, Duseja A, Chawla YK, Sharma A, Agarwal R. Lactulose improves cognitive functions and health-related quality of life in patients with cirrhosis who have minimal hepatic encephalopathy. Hepatology. 2007;45:549–559. - PubMed
-
- Sotil EU, Gottstein J, Ayala E, Randolph C, Blei AT. Impact of preoperative overt hepatic encephalopathy on neurocognitive function after liver transplantation. Liver Transpl. 2009;15:184–92. - PubMed
-
- Butterworth RF, Giguere JF, Michaud J, Lavoie J, Layrargues GP. Ammonia: key factor in the pathogenesis of hepatic encephalopathy. Neurochem Pathol. 1987;6:1–12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
