

Health disparities in staging of SEER-medicare prostate cancer patients in the United States
- PMID: 20163844
- PMCID: PMC3736596
- DOI: 10.1016/j.urology.2009.10.061
Health disparities in staging of SEER-medicare prostate cancer patients in the United States
Abstract
Objectives: To examine whether race or age disparities affected the odds of being staged among prostate cancer (PC) patients. Accurate staging is critical for determining treatment for PC.
Methods: Multivariable logistic regression models examined race and age disparities with respect to the odds of being staged among PC patients using Surveillance, Epidemiology, and End Results-Medicare data. Similar analyses were performed to estimate the adjusted odds of being staged with distant metastatic vs in situ or local/regional disease.
Results: The proportion of patients without staging ranged between 3% and 16% by age and between 6% and 8% by race. Adjusted results demonstrated statistically significant lower odds ratios (P <.05) for 70-74, 75-79, and 80+-year-olds of 0.76, 0.52, and 0.23, respectively, relative to PC patients aged 65-69. The odds of being staged for African Americans are 0.78 times that of non-Hispanic Whites (95% confidence interval = 0.72-0.86). The adjusted probability of distant metastatic disease at initial diagnosis is higher for African Americans (odds ratio = 1.61; 95% confidence interval = 1.47-1.76) and older men with odds ratios of 1.25, 1.85, and 4.33 for ages 70-74, 75-79, and 80+, respectively, compared with 65-69-year-olds (all P <.05).
Conclusions: Even though the overall odds of being staged increased over time, race and age disparities persisted. When staging did occur, the probability of distant metastatic disease was high for African Americans, and there were increasing odds of metastatic disease for all men with advanced age.
Copyright © 2010 Elsevier Inc. All rights reserved.
Figures
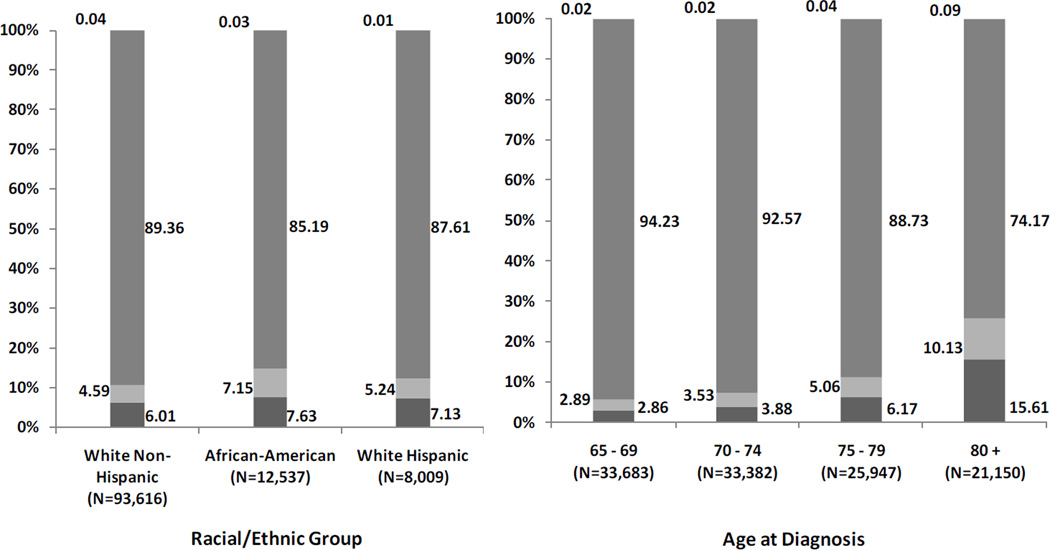
 Unstaged (N=7,158)
Unstaged (N=7,158)  Distant (N=5,609)
Distant (N=5,609)  Local/Regional (N=101,351)
Local/Regional (N=101,351)  In-situ (N=44) b Staging Distribution of Elderly SEER-Medicare Prostate Cancer Patients by Age Unstaged (N=7,158) Distant (N=5,609) Local/Regional (N=101,351) In-situ (N=44)
In-situ (N=44) b Staging Distribution of Elderly SEER-Medicare Prostate Cancer Patients by Age Unstaged (N=7,158) Distant (N=5,609) Local/Regional (N=101,351) In-situ (N=44)Comment in
-
Editorial comment.Urology. 2010 Sep;76(3):572-3. doi: 10.1016/j.urology.2009.11.017. Urology. 2010. PMID: 20832605 No abstract available.
Similar articles
-
Racial Differences in the Surgical Care of Medicare Beneficiaries With Localized Prostate Cancer.JAMA Oncol. 2016 Jan;2(1):85-93. doi: 10.1001/jamaoncol.2015.3384. JAMA Oncol. 2016. PMID: 26502115 Free PMC article.
-
Racial Disparities in the Presentation, Early Definitive Surgical Treatment, and Mortality Among Men Diagnosed with Poorly Differentiated/Undifferentiated Non-metastatic Prostate Cancer in the USA.J Racial Ethn Health Disparities. 2019 Apr;6(2):401-408. doi: 10.1007/s40615-018-00537-w. Epub 2018 Nov 30. J Racial Ethn Health Disparities. 2019. PMID: 30506310
-
Regional Variation in Active Surveillance for Low-Risk Prostate Cancer in the US.JAMA Netw Open. 2020 Dec 1;3(12):e2031349. doi: 10.1001/jamanetworkopen.2020.31349. JAMA Netw Open. 2020. PMID: 33369661 Free PMC article.
-
Mediation analyses of socioeconomic factors determining racial differences in the treatment of diffuse large B-cell lymphoma in a cohort of older adults.Medicine (Baltimore). 2019 Nov;98(46):e17960. doi: 10.1097/MD.0000000000017960. Medicine (Baltimore). 2019. PMID: 31725657 Free PMC article.
-
African-American Prostate Cancer Disparities.Curr Urol Rep. 2017 Aug 14;18(10):81. doi: 10.1007/s11934-017-0724-5. Curr Urol Rep. 2017. PMID: 28808871 Review.
Cited by
-
Racial Differences in Diffusion of Intensity-Modulated Radiation Therapy for Localized Prostate Cancer.Am J Mens Health. 2016 Sep;10(5):399-407. doi: 10.1177/1557988314568184. Epub 2015 Feb 5. Am J Mens Health. 2016. PMID: 25657192 Free PMC article.
-
African-American survivors of prostate cancer: a meta-synthesis of qualitative studies.J Cancer Surviv. 2021 Feb;15(1):40-53. doi: 10.1007/s11764-020-00909-4. Epub 2020 Jul 14. J Cancer Surviv. 2021. PMID: 32666419 Free PMC article. Review.
-
Racial variation in the cost-effectiveness of chemotherapy for prostate cancer.J Oncol Pract. 2011 May;7(3 Suppl):e16s-24s. doi: 10.1200/JOP.2011.000294. J Oncol Pract. 2011. PMID: 21886506 Free PMC article.
-
Disparities at presentation, diagnosis, treatment, and survival in African American men, affected by prostate cancer.Prostate. 2011 Jun 15;71(9):985-97. doi: 10.1002/pros.21314. Epub 2010 Dec 28. Prostate. 2011. PMID: 21541975 Free PMC article. Review.
-
Disparities With Systemic Therapies for Black Men Having Advanced Prostate Cancer: Where Do We Stand?J Clin Oncol. 2024 Jan 10;42(2):228-236. doi: 10.1200/JCO.23.00949. Epub 2023 Oct 27. J Clin Oncol. 2024. PMID: 37890125 Free PMC article. Review.
References
-
- Cohen JH, Schoenbach VJ, Kaufman JS, et al. Racial differences in clinical progression among Medicare recipients after treatment for localized prostate cancer (United States) Cancer Causes Control. 2006;17:803. - PubMed
-
- Gilligan T, Wang PS, Levin R, et al. Racial Differences in Screening for Prostate Cancer in the Elderly. Arch Intern Med. 2004;164:1858. - PubMed
-
- Byers TE, Wolf HJ, Bauer KR, et al. The impact of socioeconomic status on survival after cancer in the United States: findings from the National Program of Cancer Registries Patterns of Care Study. Cancer. 2008;113:582. - PubMed
-
- Powell IJ. Epidemiology and Pathophysiology of Prostate Cancer in African-American Men. The Journal of Urology. 2007;177:444. - PubMed
-
- Godley PA, Schenck AP, Amamoo MA, et al. Racial Differences in Mortality among Medicare Recipients after Treatment for Localized Prostate Cancer. J. Natl. Cancer Inst. 2003;95:1702. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
