

Perioperative safety in the longitudinal assessment of bariatric surgery
- PMID: 19641201
- PMCID: PMC2854565
- DOI: 10.1056/NEJMoa0901836
Perioperative safety in the longitudinal assessment of bariatric surgery
Abstract
Background: To improve decision making in the treatment of extreme obesity, the risks of bariatric surgical procedures require further characterization.
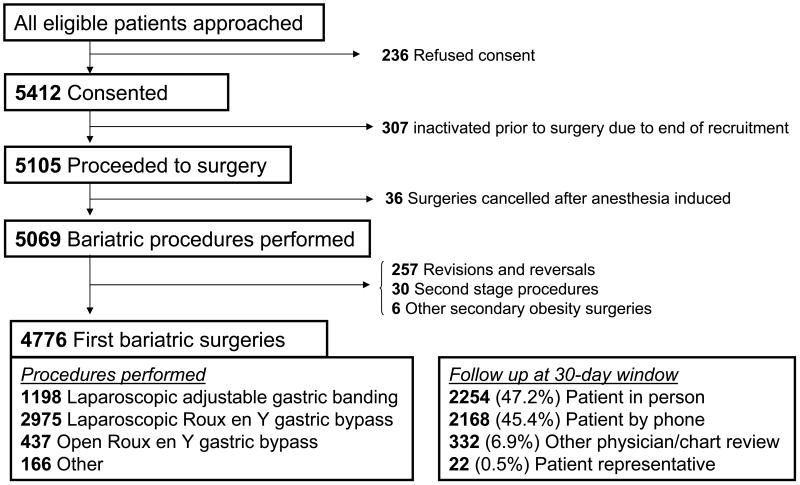
Methods: We performed a prospective, multicenter, observational study of 30-day outcomes in consecutive patients undergoing bariatric surgical procedures at 10 clinical sites in the United States from 2005 through 2007. A composite end point of 30-day major adverse outcomes (including death; venous thromboembolism; percutaneous, endoscopic, or operative reintervention; and failure to be discharged from the hospital) was evaluated among patients undergoing first-time bariatric surgery.
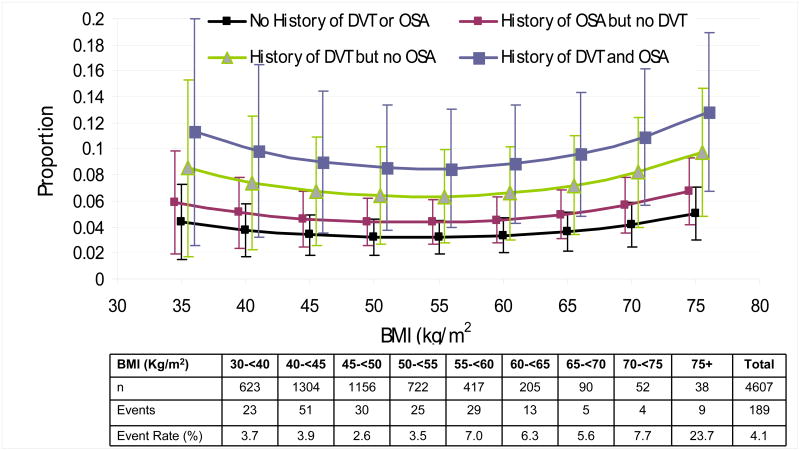
Results: There were 4776 patients who had a first-time bariatric procedure (mean age, 44.5 years; 21.1% men; 10.9% nonwhite; median body-mass index [the weight in kilograms divided by the square of the height in meters], 46.5). More than half had at least two coexisting conditions. A Roux-en-Y gastric bypass was performed in 3412 patients (with 87.2% of the procedures performed laparoscopically), and laparoscopic adjustable gastric banding was performed in 1198 patients; 166 patients underwent other procedures and were not included in the analysis. The 30-day rate of death among patients who underwent a Roux-en-Y gastric bypass or laparoscopic adjustable gastric banding was 0.3%; a total of 4.3% of patients had at least one major adverse outcome. A history of deep-vein thrombosis or pulmonary embolus, a diagnosis of obstructive sleep apnea, and impaired functional status were each independently associated with an increased risk of the composite end point. Extreme values of body-mass index were significantly associated with an increased risk of the composite end point, whereas age, sex, race, ethnic group, and other coexisting conditions were not.
Conclusions: The overall risk of death and other adverse outcomes after bariatric surgery was low and varied considerably according to patient characteristics. In helping patients make appropriate choices, short-term safety should be considered in conjunction with both the long-term effects of bariatric surgery and the risks associated with being extremely obese. (ClinicalTrials.gov number, NCT00433810.)
2009 Massachusetts Medical Society
Conflict of interest statement
Figures
Comment in
-
Surgical treatment of obesity--weighing the facts.N Engl J Med. 2009 Jul 30;361(5):520-1. doi: 10.1056/NEJMe0904837. N Engl J Med. 2009. PMID: 19641209 No abstract available.
-
Perioperative safety and bariatric surgery.N Engl J Med. 2009 Nov 5;361(19):1910; author reply 1911. doi: 10.1056/NEJMc091728. N Engl J Med. 2009. PMID: 19890138 No abstract available.
-
Perioperative safety and bariatric surgery.N Engl J Med. 2009 Nov 5;361(19):1911; author reply 1911. N Engl J Med. 2009. PMID: 19911438 No abstract available.
Similar articles
-
Metabolic acuity score: effect on major complications after bariatric surgery.Surg Obes Relat Dis. 2010 May-Jun;6(3):267-73. doi: 10.1016/j.soard.2009.09.010. Epub 2009 Sep 26. Surg Obes Relat Dis. 2010. PMID: 20005783
-
Concurrent prophylactic placement of inferior vena cava filter in gastric bypass and adjustable banding operations in the Bariatric Outcomes Longitudinal Database.J Vasc Surg. 2012 Jun;55(6):1690-5. doi: 10.1016/j.jvs.2011.12.056. Epub 2012 Feb 22. J Vasc Surg. 2012. PMID: 22360915
-
Perioperative outcomes of adolescents undergoing bariatric surgery: the Teen-Longitudinal Assessment of Bariatric Surgery (Teen-LABS) study.JAMA Pediatr. 2014 Jan;168(1):47-53. doi: 10.1001/jamapediatrics.2013.4296. JAMA Pediatr. 2014. PMID: 24189578 Free PMC article. Clinical Trial.
-
Gastric banding or bypass? A systematic review comparing the two most popular bariatric procedures.Am J Med. 2008 Oct;121(10):885-93. doi: 10.1016/j.amjmed.2008.05.036. Am J Med. 2008. PMID: 18823860 Review.
-
The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation.Health Technol Assess. 2009 Sep;13(41):1-190, 215-357, iii-iv. doi: 10.3310/hta13410. Health Technol Assess. 2009. PMID: 19726018 Review.
Cited by
-
Management of Excessive Weight Loss Following Laparoscopic Roux-en-Y Gastric Bypass: Clinical Algorithm and Surgical Techniques.Obes Surg. 2016 Jan;26(1):5-11. doi: 10.1007/s11695-015-1775-7. Obes Surg. 2016. PMID: 26105983
-
Expectations for weight loss and willingness to accept risk among patients seeking weight loss surgery.JAMA Surg. 2013 Mar;148(3):264-71. doi: 10.1001/jamasurg.2013.1048. JAMA Surg. 2013. PMID: 23553327 Free PMC article.
-
Bariatric surgery outcomes in patients aged 65 years and older at an American Society for Metabolic and Bariatric Surgery Center of Excellence.Obes Surg. 2010 Sep;20(9):1199-205. doi: 10.1007/s11695-010-0201-4. Obes Surg. 2010. PMID: 20532834
-
Anastomotic leak test using indocyanine green during laparoscopic Roux-en-Y gastric bypass: A cohort study.Ann Med Surg (Lond). 2022 Nov 17;84:104939. doi: 10.1016/j.amsu.2022.104939. eCollection 2022 Dec. Ann Med Surg (Lond). 2022. PMID: 36536736 Free PMC article.
-
Surgery: how safe is bariatric surgery?Nat Rev Endocrinol. 2009 Dec;5(12):645-6. doi: 10.1038/nrendo.2009.221. Nat Rev Endocrinol. 2009. PMID: 19924147 No abstract available.
References
-
- Dixon JB, et al. Adjustable gastric banding and conventional therapy for type 2 diabetes: a randomized controlled trial. JAMA. 2008;299(3):316–23. - PubMed
-
- Sjostrom L, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351(26):2683–93. - PubMed
-
- Sjostrom L, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357(8):741–52. - PubMed
-
- Adams TD, et al. Long-term mortality after gastric bypass surgery. N Engl J Med. 2007;357(8):753–61. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U01 DK066585-05/DK/NIDDK NIH HHS/United States
- U01 DK066555/DK/NIDDK NIH HHS/United States
- U01-DK66526/DK/NIDDK NIH HHS/United States
- M01RR-00037/RR/NCRR NIH HHS/United States
- U01 DK066526/DK/NIDDK NIH HHS/United States
- U01 DK066557-05/DK/NIDDK NIH HHS/United States
- U01 DK066555-05/DK/NIDDK NIH HHS/United States
- U01 DK066471-05/DK/NIDDK NIH HHS/United States
- U01-DK66568/DK/NIDDK NIH HHS/United States
- U01 DK066471/DK/NIDDK NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- U01 DK066568-05/DK/NIDDK NIH HHS/United States
- U01 DK066526-05/DK/NIDDK NIH HHS/United States
- U01 DK066585/DK/NIDDK NIH HHS/United States
- U01 DK066557/DK/NIDDK NIH HHS/United States
- U01 DK066568/DK/NIDDK NIH HHS/United States
- M01 RR000037/RR/NCRR NIH HHS/United States
- U01-DK066557/DK/NIDDK NIH HHS/United States
- U01-DK66471/DK/NIDDK NIH HHS/United States
- U01-DK66585/DK/NIDDK NIH HHS/United States
- U01-DK66667/DK/NIDDK NIH HHS/United States
- U01 DK066667-05/DK/NIDDK NIH HHS/United States
- U01-DK66555/DK/NIDDK NIH HHS/United States
- U01 DK066667/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials