

RNA viruses in community-acquired childhood pneumonia in semi-urban Nepal; a cross-sectional study
- PMID: 19635124
- PMCID: PMC2727531
- DOI: 10.1186/1741-7015-7-35
RNA viruses in community-acquired childhood pneumonia in semi-urban Nepal; a cross-sectional study
Abstract
Background: Pneumonia is among the main causes of illness and death in children <5 years of age. There is a need to better describe the epidemiology of viral community-acquired pneumonia (CAP) in developing countries.
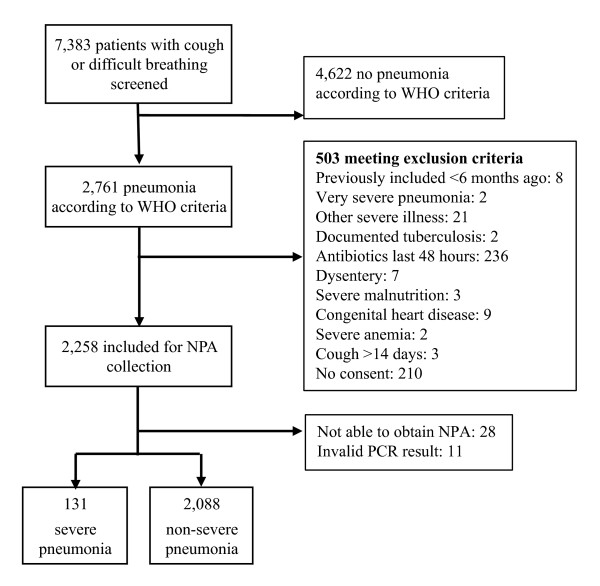
Methods: From July 2004 to June 2007, we examined nasopharyngeal aspirates (NPA) from 2,230 cases of pneumonia (World Health Organization criteria) in children 2 to 35 months old recruited in a randomized trial of zinc supplementation at a field clinic in Bhaktapur, Nepal. The specimens were examined for respiratory syncytial virus (RSV), influenza virus type A (InfA) and B (InfB), parainfluenza virus types 1, 2 and 3 (PIV1, PIV2, and PIV3), and human metapneumovirus (hMPV) using a multiplex reverse transcriptase polymerase chain reaction (PCR) assay.
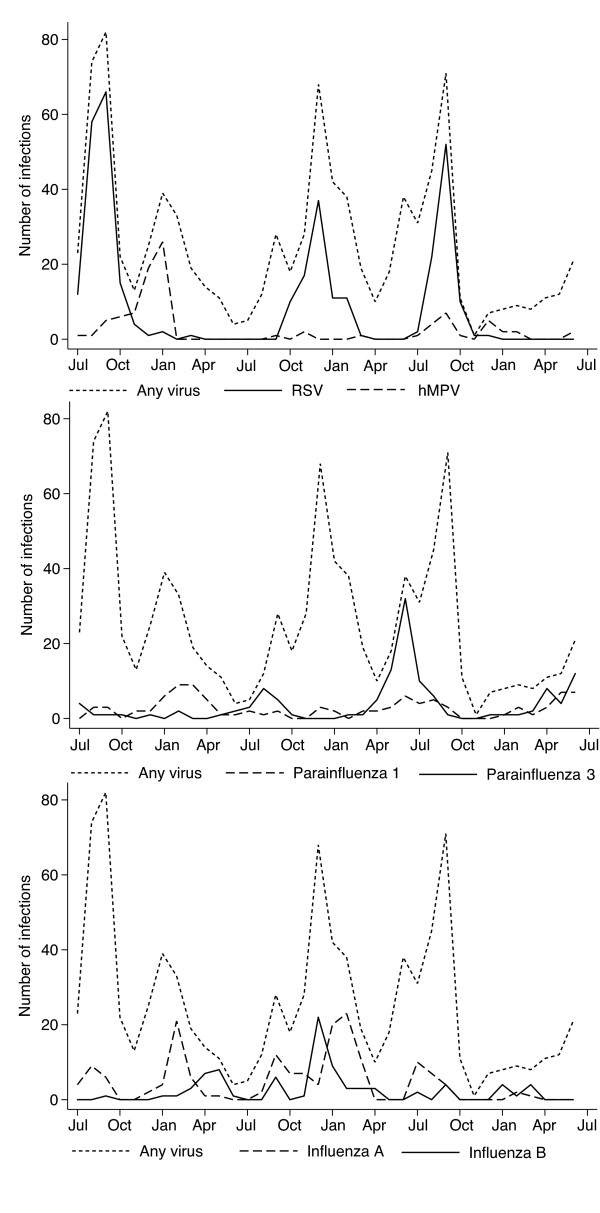
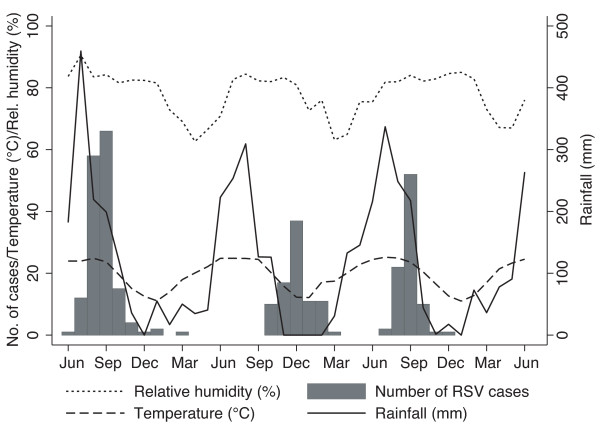
Results: We identified 919 virus isolates in 887 (40.0%) of the 2,219 NPA specimens with a valid PCR result, of which 334 (15.1%) yielded RSV, 164 (7.4%) InfA, 129 (5.8%) PIV3, 98 (4.4%) PIV1, 93 (4.2%) hMPV, 84 (3.8%) InfB, and 17 (0.8%) PIV2. CAP occurred in an epidemic pattern with substantial temporal variation during the three years of study. The largest peaks of pneumonia occurrence coincided with peaks of RSV infection, which occurred in epidemics during the rainy season and in winter. The monthly number of RSV infections was positively correlated with relative humidity (rs = 0.40, P = 0.01), but not with temperature or rainfall. An hMPV epidemic occurred during one of the three winter seasons and the monthly number of hMPV cases was also associated with relative humidity (rs = 0.55, P = 0.0005).
Conclusion: Respiratory RNA viruses were detected from NPA in 40% of CAP cases in our study. The most commonly isolated viruses were RSV, InfA, and PIV3. RSV infections contributed substantially to the observed CAP epidemics. The occurrence of viral CAP in this community seemed to reflect more or less overlapping micro-epidemics with several respiratory viruses, highlighting the challenges of developing and implementing effective public health control measures.
Figures

Similar articles
-
CAUSATIVE AGENTS OF SEVERE COMMUNITY ACQUIRED VIRAL PNEUMONIA AMONG CHILDREN IN EASTERN THAILAND.Southeast Asian J Trop Med Public Health. 2015 Jul;46(4):650-6. Southeast Asian J Trop Med Public Health. 2015. PMID: 26867384
-
Clinical presentation and severity of viral community-acquired pneumonia in young Nepalese children.Pediatr Infect Dis J. 2010 Jan;29(1):e1-6. doi: 10.1097/INF.0b013e3181c2a1b9. Pediatr Infect Dis J. 2010. PMID: 19935451
-
RNA viruses in young Nepalese children hospitalized with severe pneumonia.Pediatr Infect Dis J. 2011 Dec;30(12):1032-6. doi: 10.1097/INF.0b013e31822f845f. Pediatr Infect Dis J. 2011. PMID: 21860338
-
Systematic review of respiratory viral pathogens identified in adults with community-acquired pneumonia in Europe.J Clin Virol. 2017 Oct;95:26-35. doi: 10.1016/j.jcv.2017.07.019. Epub 2017 Aug 5. J Clin Virol. 2017. PMID: 28837859 Free PMC article. Review.
-
Viral pneumonia in adults and older children in sub-Saharan Africa - epidemiology, aetiology, diagnosis and management.Pneumonia (Nathan). 2014 Dec 1;5(Suppl 1):18-29. doi: 10.15172/pneu.2014.5/446. eCollection 2014. Pneumonia (Nathan). 2014. PMID: 31641571 Free PMC article. Review.
Cited by
-
Viral etiology of influenza-like illnesses in Antananarivo, Madagascar, July 2008 to June 2009.PLoS One. 2011 Mar 3;6(3):e17579. doi: 10.1371/journal.pone.0017579. PLoS One. 2011. PMID: 21390235 Free PMC article.
-
Respiratory syncytial virus infection in infants in rural Nepal.J Infect. 2016 Aug;73(2):145-54. doi: 10.1016/j.jinf.2016.05.007. Epub 2016 May 27. J Infect. 2016. PMID: 27241525 Free PMC article.
-
Cytokine Concentrations in Plasma from Children with Severe and Non-Severe Community Acquired Pneumonia.PLoS One. 2015 Sep 25;10(9):e0138978. doi: 10.1371/journal.pone.0138978. eCollection 2015. PLoS One. 2015. PMID: 26407163 Free PMC article. Clinical Trial.
-
Seasonal distribution and epidemiological characteristics of human metapneumovirus infections in pediatric inpatients in Southeast China.Arch Virol. 2013 Feb;158(2):417-24. doi: 10.1007/s00705-012-1492-7. Epub 2012 Oct 17. Arch Virol. 2013. PMID: 23074040 Free PMC article.
-
Chinese medicinal herbs for childhood pneumonia: a systematic review of effectiveness and safety.Evid Based Complement Alternat Med. 2013;2013:203845. doi: 10.1155/2013/203845. Epub 2013 Mar 10. Evid Based Complement Alternat Med. 2013. PMID: 23554826 Free PMC article.
References
-
- Berman S. Epidemiology of acute respiratory infections in children of developing countries. Rev Infect Dis. 1991. pp. S454–462. - PubMed
-
- Iwane MK, Edwards KM, Szilagyi PG, Walker FJ, Griffin MR, Weinberg GA, Coulen C, Poehling KA, Shone LP, Balter S, Hall CB, Erdman DD, Wooten K, Schwartz B. Population-based surveillance for hospitalizations associated with respiratory syncytial virus, influenza virus, and parainfluenza viruses among young children. Pediatrics. 2004;113:1758–1764. doi: 10.1542/peds.113.6.1758. - DOI - PubMed
-
- Henrickson KJ, Hoover S, Kehl KS, Hua W. National disease burden of respiratory viruses detected in children by polymerase chain reaction. Pediatr Infect Dis J. 2004. pp. S11–18. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
