

Timing of initiation of antiretroviral therapy in AIDS-free HIV-1-infected patients: a collaborative analysis of 18 HIV cohort studies
- PMID: 19361855
- PMCID: PMC2670965
- DOI: 10.1016/S0140-6736(09)60612-7
Timing of initiation of antiretroviral therapy in AIDS-free HIV-1-infected patients: a collaborative analysis of 18 HIV cohort studies
Abstract
Background: The CD4 cell count at which combination antiretroviral therapy should be started is a central, unresolved issue in the care of HIV-1-infected patients. In the absence of randomised trials, we examined this question in prospective cohort studies.
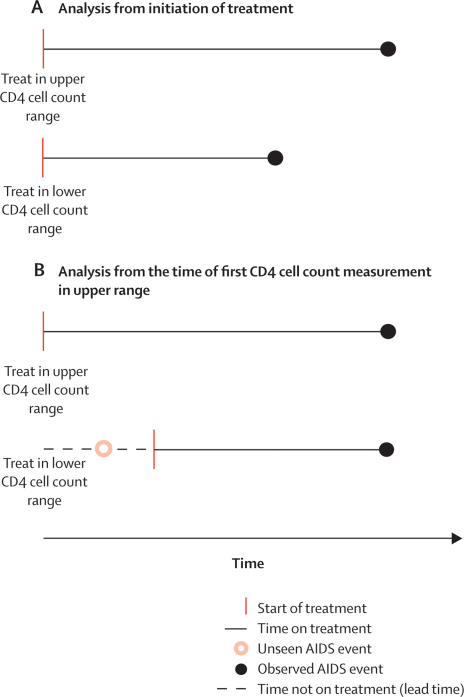
Methods: We analysed data from 18 cohort studies of patients with HIV. Antiretroviral-naive patients from 15 of these studies were eligible for inclusion if they had started combination antiretroviral therapy (while AIDS-free, with a CD4 cell count less than 550 cells per microL, and with no history of injecting drug use) on or after Jan 1, 1998. We used data from patients followed up in seven of the cohorts in the era before the introduction of combination therapy (1989-95) to estimate distributions of lead times (from the first CD4 cell count measurement in an upper range to the upper threshold of a lower range) and unseen AIDS and death events (occurring before the upper threshold of a lower CD4 cell count range is reached) in the absence of treatment. These estimations were used to impute completed datasets in which lead times and unseen AIDS and death events were added to data for treated patients in deferred therapy groups. We compared the effect of deferred initiation of combination therapy with immediate initiation on rates of AIDS and death, and on death alone, in adjacent CD4 cell count ranges of width 100 cells per microL.
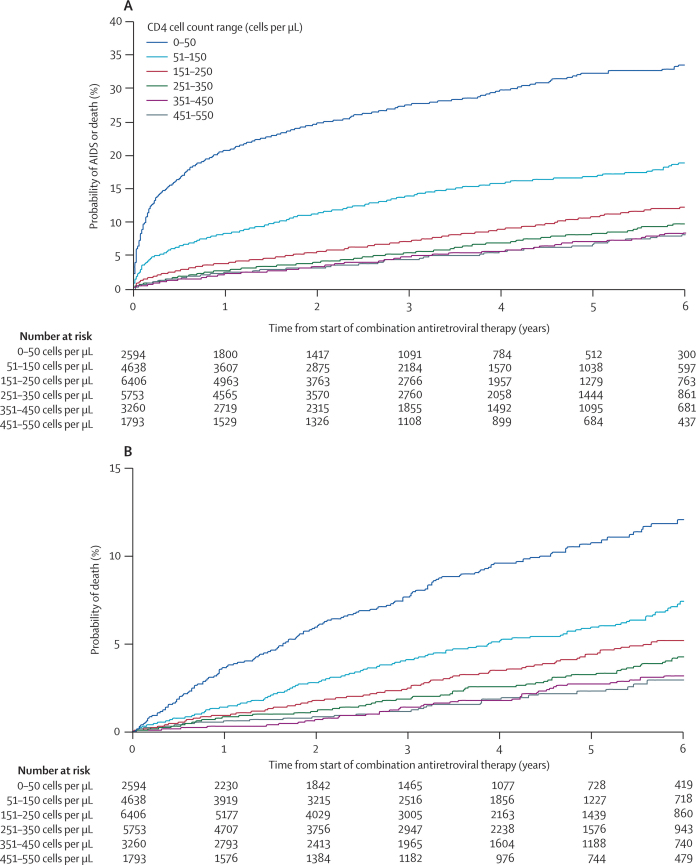
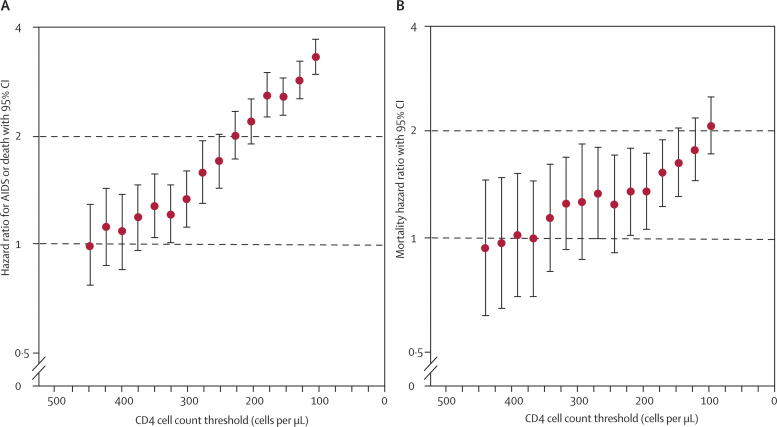
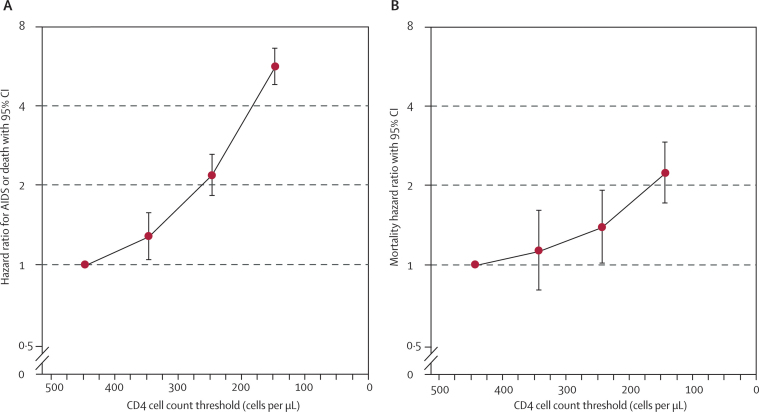
Findings: Data were obtained for 21 247 patients who were followed up during the era before the introduction of combination therapy and 24 444 patients who were followed up from the start of treatment. Deferring combination therapy until a CD4 cell count of 251-350 cells per microL was associated with higher rates of AIDS and death than starting therapy in the range 351-450 cells per microL (hazard ratio [HR] 1.28, 95% CI 1.04-1.57). The adverse effect of deferring treatment increased with decreasing CD4 cell count threshold. Deferred initiation of combination therapy was also associated with higher mortality rates, although effects on mortality were less marked than effects on AIDS and death (HR 1.13, 0.80-1.60, for deferred initiation of treatment at CD4 cell count 251-350 cells per microL compared with initiation at 351-450 cells per microL).
Interpretation: Our results suggest that 350 cells per microL should be the minimum threshold for initiation of antiretroviral therapy, and should help to guide physicians and patients in deciding when to start treatment.
Figures
Comment in
-
Should the CD4 threshold for starting ART be raised?Lancet. 2009 Apr 18;373(9672):1314-6. doi: 10.1016/S0140-6736(09)60654-1. Epub 2009 Apr 8. Lancet. 2009. PMID: 19361856 No abstract available.
Similar articles
-
[Timing of initiation of antiretroviral therapy in HIV-1-infected patients. Meta-analysis of the When To Start Consortium].Internist (Berl). 2010 Apr;51(4):539-41. doi: 10.1007/s00108-010-2592-7. Internist (Berl). 2010. PMID: 20237749 German. No abstract available.
-
Prognostic importance of initial response in HIV-1 infected patients starting potent antiretroviral therapy: analysis of prospective studies.Lancet. 2003 Aug 30;362(9385):679-86. doi: 10.1016/s0140-6736(03)14229-8. Lancet. 2003. PMID: 12957089
-
Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies.Lancet. 2002 Jul 13;360(9327):119-29. doi: 10.1016/s0140-6736(02)09411-4. Lancet. 2002. PMID: 12126821
-
Optimal time for initiation of antiretroviral therapy in asymptomatic, HIV-infected, treatment-naive adults.Cochrane Database Syst Rev. 2010 Mar 17;2010(3):CD008272. doi: 10.1002/14651858.CD008272.pub2. Cochrane Database Syst Rev. 2010. PMID: 20238364 Free PMC article. Review.
-
Optimal time for initiating antiretroviral therapy (ART) in HIV-infected, treatment-naive children aged 2 to 5 years old.Cochrane Database Syst Rev. 2013 Oct 10;10(10):CD010309. doi: 10.1002/14651858.CD010309.pub2. Cochrane Database Syst Rev. 2013. PMID: 24114324 Free PMC article. Review.
Cited by
-
Improving HIV outcomes in resource-limited countries: the importance of quality indicators.BMC Health Serv Res. 2012 Nov 24;12:427. doi: 10.1186/1472-6963-12-427. BMC Health Serv Res. 2012. PMID: 23176556 Free PMC article.
-
Service integration: opportunities to expand access to antiretroviral therapy for people who inject drugs in Tanzania.J Int AIDS Soc. 2015 Jul 21;18(1):19936. doi: 10.7448/IAS.18.1.19936. eCollection 2015. J Int AIDS Soc. 2015. PMID: 26202669 Free PMC article. No abstract available.
-
Innovative Strategies for Scale up of Effective Combination HIV Prevention Interventions in Sub-Saharan Africa.Curr HIV/AIDS Rep. 2015 Jun;12(2):231-7. doi: 10.1007/s11904-015-0262-z. Curr HIV/AIDS Rep. 2015. PMID: 25929960 Review.
-
Gender differences in immune reconstitution: a multicentric cohort analysis in sub-Saharan Africa.PLoS One. 2012;7(2):e31078. doi: 10.1371/journal.pone.0031078. Epub 2012 Feb 17. PLoS One. 2012. PMID: 22363550 Free PMC article.
-
Antiretroviral therapy improves survival among TB-HIV co-infected patients who have CD4+ T-cell count above 350cells/mm3.BMC Infect Dis. 2016 Oct 17;16(1):572. doi: 10.1186/s12879-016-1916-1. BMC Infect Dis. 2016. PMID: 27751168 Free PMC article.
References
-
- Palella FJ, Delaney KM, Moorman AC. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. N Engl J Med. 1998;338:853–908. - PubMed
-
- Hammer SM, Squires KE, Hughes MD. A controlled trial of two nucleoside analogues plus indinavir in persons with human immunodeficiency virus infection and CD4 cell counts of 200 per cubic millimeter or less. N Engl J Med. 1997;337:725–733. - PubMed
-
- Cole SR, Hernan MA, Robins JM. Effect of highly active antiretroviral therapy on time to acquired immunodeficiency syndrome or death using marginal structural models. Am J Epidemiol. 2003;158:687–694. - PubMed
-
- Sterne JAC, Hernan MA, Ledergerber B. Long-term effectiveness of potent antiretroviral therapy in preventing AIDS and death: a prospective cohort study. Lancet. 2005;366:378–384. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
