

The incidence of co-morbidities related to obesity and overweight: a systematic review and meta-analysis
- PMID: 19320986
- PMCID: PMC2667420
- DOI: 10.1186/1471-2458-9-88
The incidence of co-morbidities related to obesity and overweight: a systematic review and meta-analysis
Abstract
Background: Overweight and obese persons are at risk of a number of medical conditions which can lead to further morbidity and mortality. The primary objective of this study is to provide an estimate of the incidence of each co-morbidity related to obesity and overweight using a meta-analysis.
Methods: A literature search for the twenty co-morbidities identified in a preliminary search was conducted in Medline and Embase (Jan 2007). Studies meeting the inclusion criteria (prospective cohort studies of sufficient size reporting risk estimate based on the incidence of disease) were extracted. Study-specific unadjusted relative risks (RRs) on the log scale comparing overweight with normal and obese with normal were weighted by the inverse of their corresponding variances to obtain a pooled RR with 95% confidence intervals (CI).
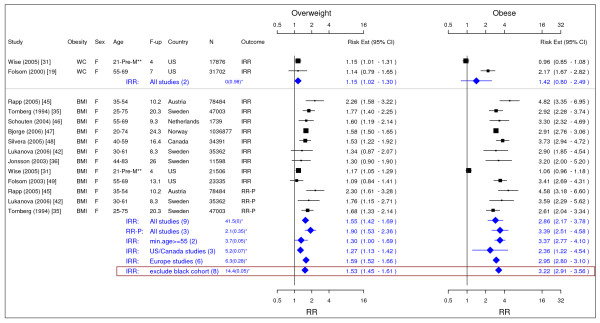
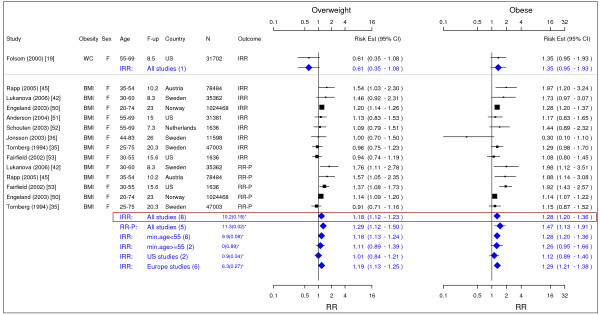
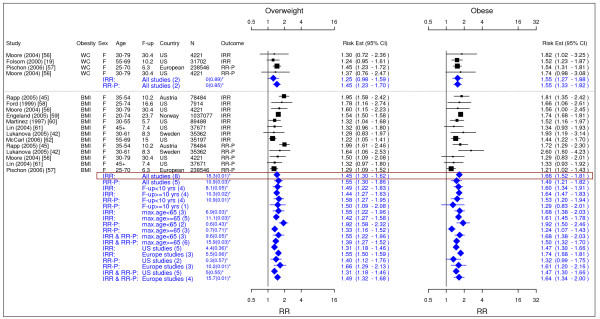
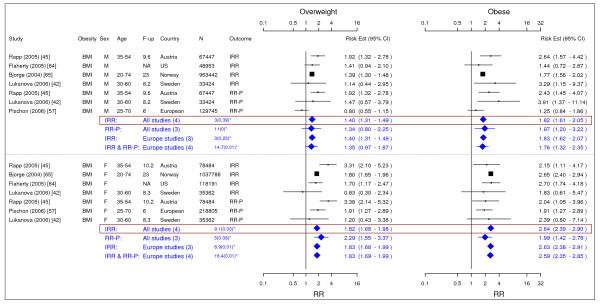
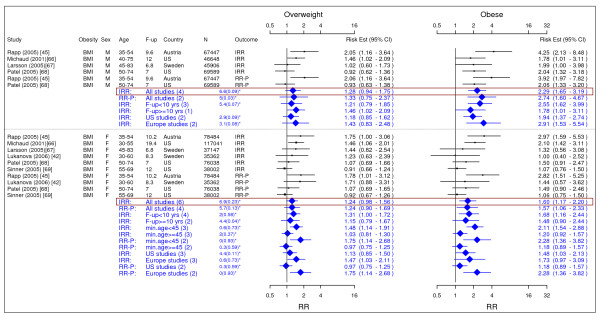
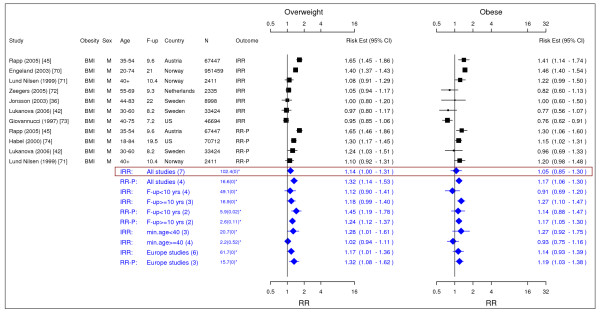
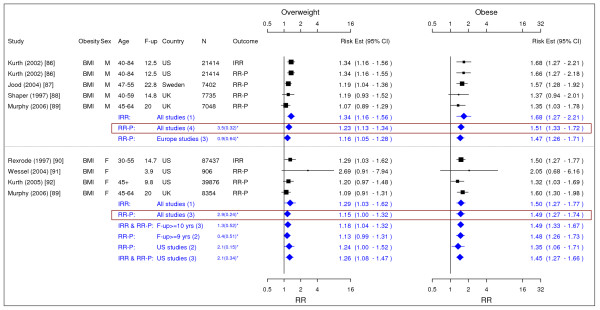
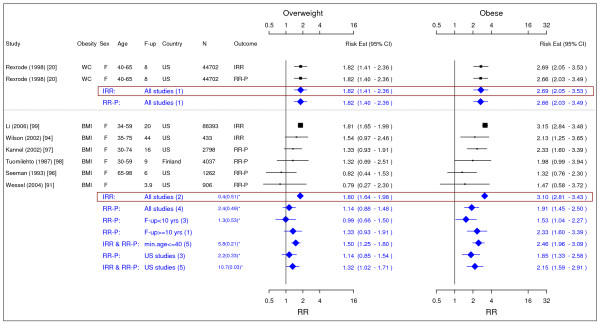
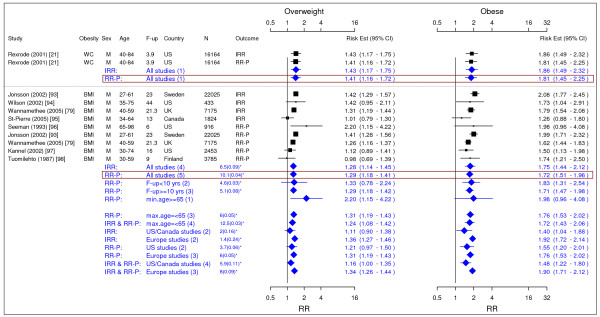
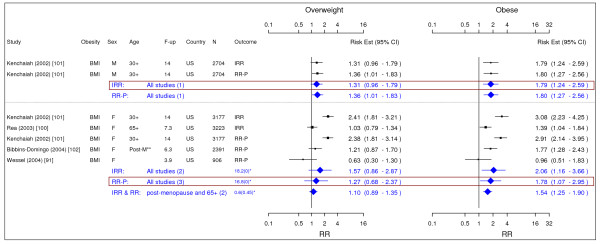
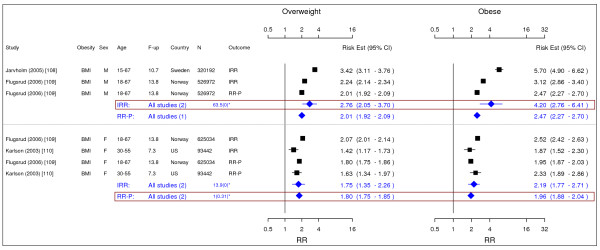
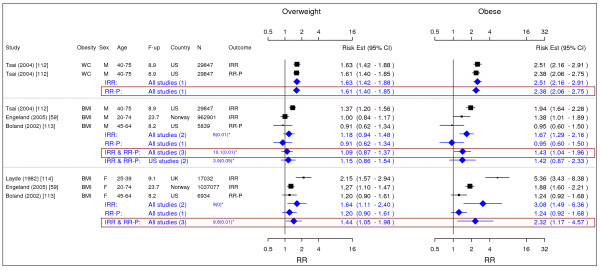
Results: A total of 89 relevant studies were identified. The review found evidence for 18 co-morbidities which met the inclusion criteria. The meta-analysis determined statistically significant associations for overweight with the incidence of type II diabetes, all cancers except esophageal (female), pancreatic and prostate cancer, all cardiovascular diseases (except congestive heart failure), asthma, gallbladder disease, osteoarthritis and chronic back pain. We noted the strongest association between overweight defined by body mass index (BMI) and the incidence of type II diabetes in females (RR = 3.92 (95% CI: 3.10-4.97)). Statistically significant associations with obesity were found with the incidence of type II diabetes, all cancers except esophageal and prostate cancer, all cardiovascular diseases, asthma, gallbladder disease, osteoarthritis and chronic back pain. Obesity defined by BMI was also most strongly associated with the incidence of type II diabetes in females (12.41 (9.03-17.06)).
Conclusion: Both overweight and obesity are associated with the incidence of multiple co-morbidities including type II diabetes, cancer and cardiovascular diseases. Maintenance of a healthy weight could be important in the prevention of the large disease burden in the future. Further studies are needed to explore the biological mechanisms that link overweight and obesity with these co-morbidities.
Figures






Similar articles
-
Behavioral and Pharmacotherapy Weight Loss Interventions to Prevent Obesity-Related Morbidity and Mortality in Adults: An Updated Systematic Review for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Sep. Report No.: 18-05239-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Sep. Report No.: 18-05239-EF-1. PMID: 30354042 Free Books & Documents. Review.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
The effectiveness of web-based programs on the reduction of childhood obesity in school-aged children: A systematic review.JBI Libr Syst Rev. 2012;10(42 Suppl):1-14. doi: 10.11124/jbisrir-2012-248. JBI Libr Syst Rev. 2012. PMID: 27820152
-
Chronic disease burden associated with overweight and obesity in Ireland: the effects of a small BMI reduction at population level.BMC Public Health. 2014 Feb 10;14:143. doi: 10.1186/1471-2458-14-143. BMC Public Health. 2014. PMID: 24512151 Free PMC article.
-
Association of weight status and the risks of diabetes in adults: a systematic review and meta-analysis of prospective cohort studies.Int J Obes (Lond). 2022 Jun;46(6):1101-1113. doi: 10.1038/s41366-022-01096-1. Epub 2022 Feb 23. Int J Obes (Lond). 2022. PMID: 35197569 Review.
Cited by
-
Assessing the evidence for health benefits of low-level weight loss: a systematic review.Int J Obes (Lond). 2024 Nov 1. doi: 10.1038/s41366-024-01664-7. Online ahead of print. Int J Obes (Lond). 2024. PMID: 39487296 Review.
-
The Weight on Sight: Exploring the Links Between Obesity and Ocular Diseases.Cureus. 2024 Oct 30;16(10):e72742. doi: 10.7759/cureus.72742. eCollection 2024 Oct. Cureus. 2024. PMID: 39483584 Free PMC article. Review.
-
U.S. weight trends: a longitudinal analysis of an NIH-partnered dataset.Int J Obes (Lond). 2024 Oct 29. doi: 10.1038/s41366-024-01661-w. Online ahead of print. Int J Obes (Lond). 2024. PMID: 39472690
-
Association between body mass index and urinary tract infections: A cross-sectional investigation of the PERSIAN Guilan cohort study.Obes Sci Pract. 2024 Oct 19;10(5):e70013. doi: 10.1002/osp4.70013. eCollection 2024 Oct. Obes Sci Pract. 2024. PMID: 39429540 Free PMC article.
-
You Eat with Your Eyes: Framing of Food Choice Options Affects Decision Conflict and Visual Attention in Food Choice Task.Nutrients. 2024 Oct 1;16(19):3343. doi: 10.3390/nu16193343. Nutrients. 2024. PMID: 39408310 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
