

Human coronavirus and acute respiratory illness in older adults with chronic obstructive pulmonary disease
- PMID: 19239338
- PMCID: PMC7110218
- DOI: 10.1086/597122
Human coronavirus and acute respiratory illness in older adults with chronic obstructive pulmonary disease
Abstract
Background: The clinical features and incidence of human coronavirus (HCoV) infections in chronically ill older adults need better definition.
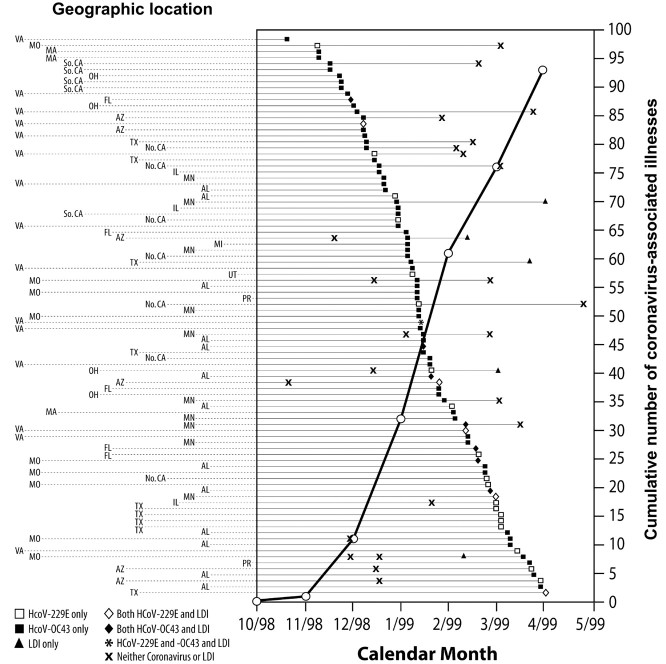
Methods: HCoV infection was determined on the basis of a 4-fold increase in serum antibody and the detection of HCoV by reverse-transcription polymerase chain reaction. Laboratory-documented influenza (LDI) was detected by serologic assay and culture. HCoV illnesses were compared with other acute respiratory illnesses identified by active surveillance, during the 1998-99 winter respiratory-virus season, of 2215 patients with chronic obstructive pulmonary disease who were > or = 50 years old and who received influenza vaccines.
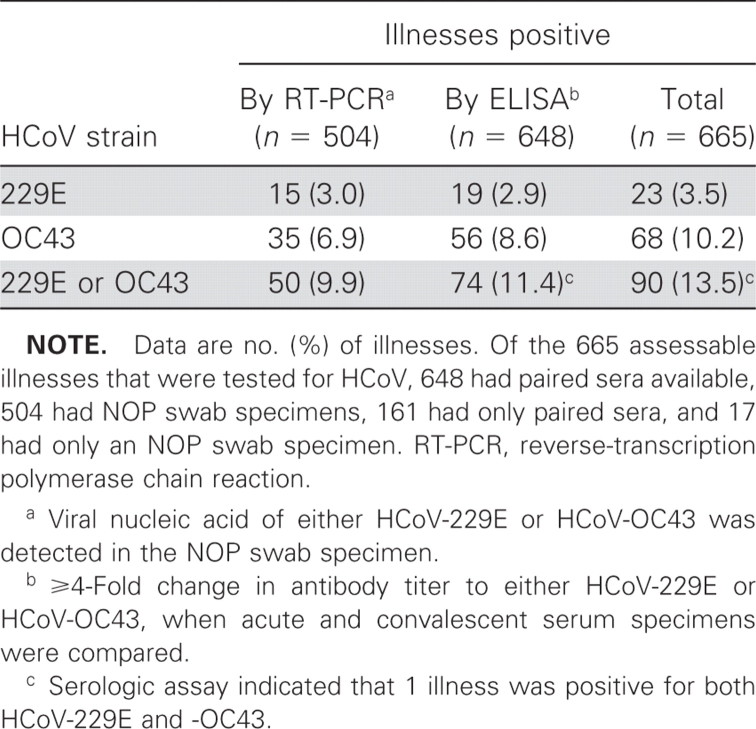
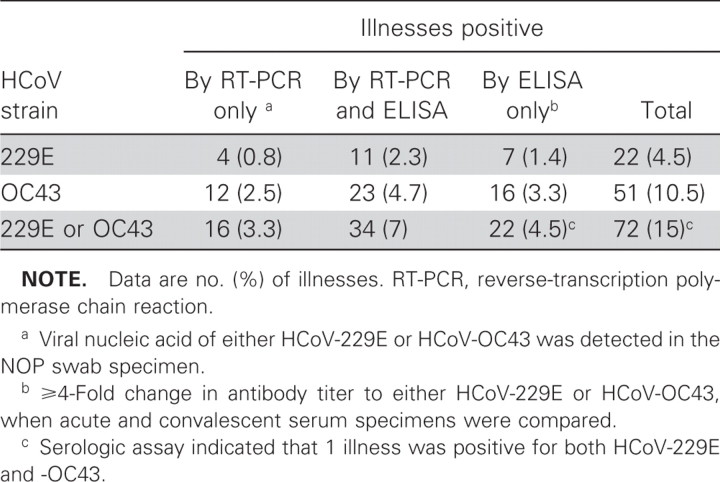
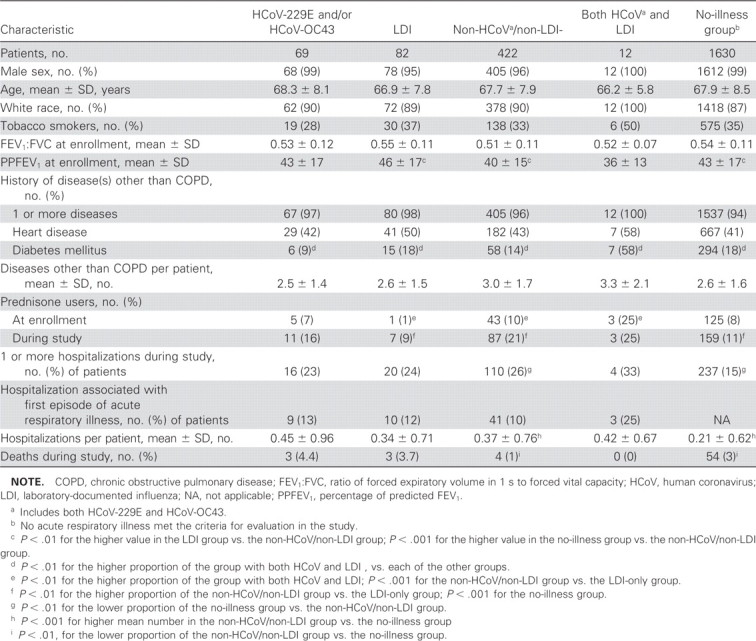
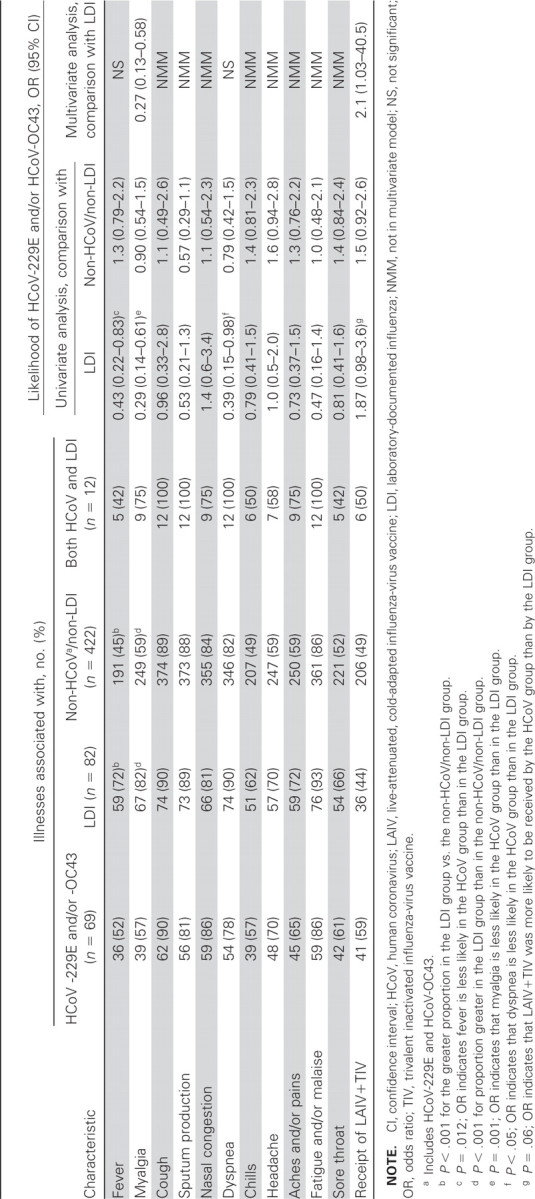
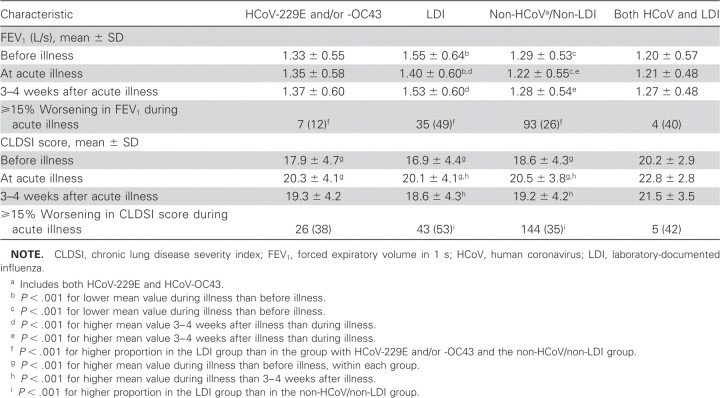
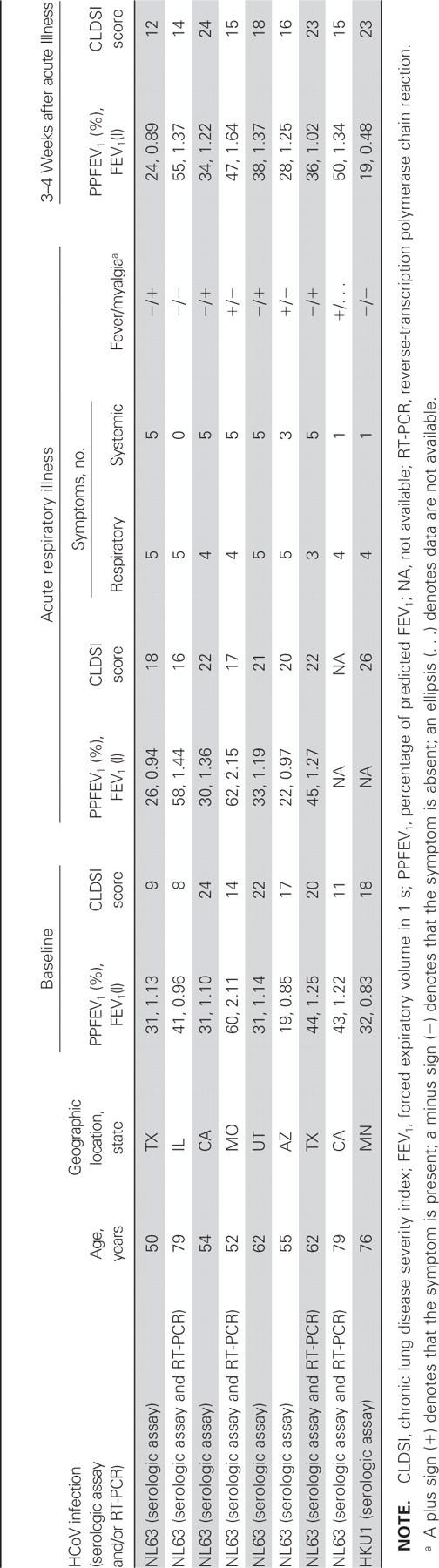
Results: HCoV-229E and HCoV-OC43 were associated with 90 (14%) of 665 illnesses (HCoV-229E in 22, HCoV-OC43 in 67, and both in 1), LDI with 107 (16%) of 678 illnesses. In multivariate logistic regression analysis, myalgia was less likely with HCoV infection than with LDI (OR, 0.27 [95% confidence limit, 0.13-0.58]). A majority of these HCoV and LDI illnesses exhibited each of 11 symptoms and signs of acute respiratory illness. Spirometric results worsened most often with LDI, and many acute respiratory illnesses, regardless of etiology, were associated with hospitalization. A total of 8 illnesses were associated with HCoV-NL63, 1 with HCoV-HKU1.
Conclusions: The frequencies of HCoV and LDI illnesses were similar. HCoV illness was less severe than LDI illness, was accompanied by multiple respiratory and systemic symptoms, and was associated with hospitalization.
Figures
Similar articles
-
Prevalence of antibodies to four human coronaviruses is lower in nasal secretions than in serum.Clin Vaccine Immunol. 2010 Dec;17(12):1875-80. doi: 10.1128/CVI.00278-10. Epub 2010 Oct 13. Clin Vaccine Immunol. 2010. PMID: 20943876 Free PMC article.
-
Genetic variability of human coronavirus OC43-, 229E-, and NL63-like strains and their association with lower respiratory tract infections of hospitalized infants and immunocompromised patients.J Med Virol. 2006 Jul;78(7):938-49. doi: 10.1002/jmv.20645. J Med Virol. 2006. PMID: 16721849 Free PMC article.
-
Coronavirus HKU1 and other coronavirus infections in Hong Kong.J Clin Microbiol. 2006 Jun;44(6):2063-71. doi: 10.1128/JCM.02614-05. J Clin Microbiol. 2006. PMID: 16757599 Free PMC article.
-
Coronavirus Occurrence in the Household Influenza Vaccine Evaluation (HIVE) Cohort of Michigan Households: Reinfection Frequency and Serologic Responses to Seasonal and Severe Acute Respiratory Syndrome Coronaviruses.J Infect Dis. 2021 Jul 2;224(1):49-59. doi: 10.1093/infdis/jiab161. J Infect Dis. 2021. PMID: 33755731 Free PMC article.
-
[Coronaviruses as the cause of respiratory infections].Internist (Berl). 2019 Nov;60(11):1136-1145. doi: 10.1007/s00108-019-00671-5. Internist (Berl). 2019. PMID: 31455974 Free PMC article. Review. German.
Cited by
-
Cross-immunity between respiratory coronaviruses may limit COVID-19 fatalities.Med Hypotheses. 2020 Nov;144:110049. doi: 10.1016/j.mehy.2020.110049. Epub 2020 Jun 30. Med Hypotheses. 2020. PMID: 32758887 Free PMC article.
-
Co-circulation of four human coronaviruses (HCoVs) in Queensland children with acute respiratory tract illnesses in 2004.Viruses. 2012 Apr;4(4):637-53. doi: 10.3390/v4040637. Epub 2012 Apr 23. Viruses. 2012. PMID: 22590689 Free PMC article.
-
Respiratory syncytial virus-associated illness in adults with advanced chronic obstructive pulmonary disease and/or congestive heart failure.J Med Virol. 2019 Jan;91(1):65-71. doi: 10.1002/jmv.25285. Epub 2018 Sep 24. J Med Virol. 2019. PMID: 30132922 Free PMC article.
-
The influence of virus infections on the course of COPD.Eur J Microbiol Immunol (Bp). 2012 Sep;2(3):176-85. doi: 10.1556/EuJMI.2.2012.3.2. Epub 2012 Sep 10. Eur J Microbiol Immunol (Bp). 2012. PMID: 24688763 Free PMC article. Review.
-
COVID-19 Susceptibility in chronic obstructive pulmonary disease.Eur J Clin Invest. 2020 Oct;50(10):e13382. doi: 10.1111/eci.13382. Epub 2020 Sep 2. Eur J Clin Invest. 2020. PMID: 32780415 Free PMC article. Review.
References
-
- McIntosh K, Anderson LJ. Coronaviruses, including severe acute respiratory syndrome (SARS)-associated coronavirus. In: Principles and practice of infectious diseases, 6th ed. Vol 2., editors; Mandell GL, Bennett JE, Dolin R, editors. Principles and practice of infectious diseases. 6th ed. Philadelphia: Elsevier Churchill Livingstone; 2005. pp. 1990–7.
-
- Lee N, Hui D, Wu A, et al. A major outbreak of severe acute respiratory syndrome in Hong Kong. N Engl J Med. 2003;348:1986–94. - PubMed
-
- Peiris JSM, Yuen KY, Osterhaus ADME, Stöhr K. The severe acute respiratory syndrome. N Engl J Med. 2003;349:2431–41. - PubMed
-
- Gump DW, Phillips CA, Forsyth BR, McIntosh K, Lamborn KR. Role of infection in chronic bronchitis. Am Rev Respir Dis. 1976;113:465–74. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
