

Patient adherence in COPD
- PMID: 18728206
- PMCID: PMC4747423
- DOI: 10.1136/thx.2007.086041
Patient adherence in COPD
Abstract
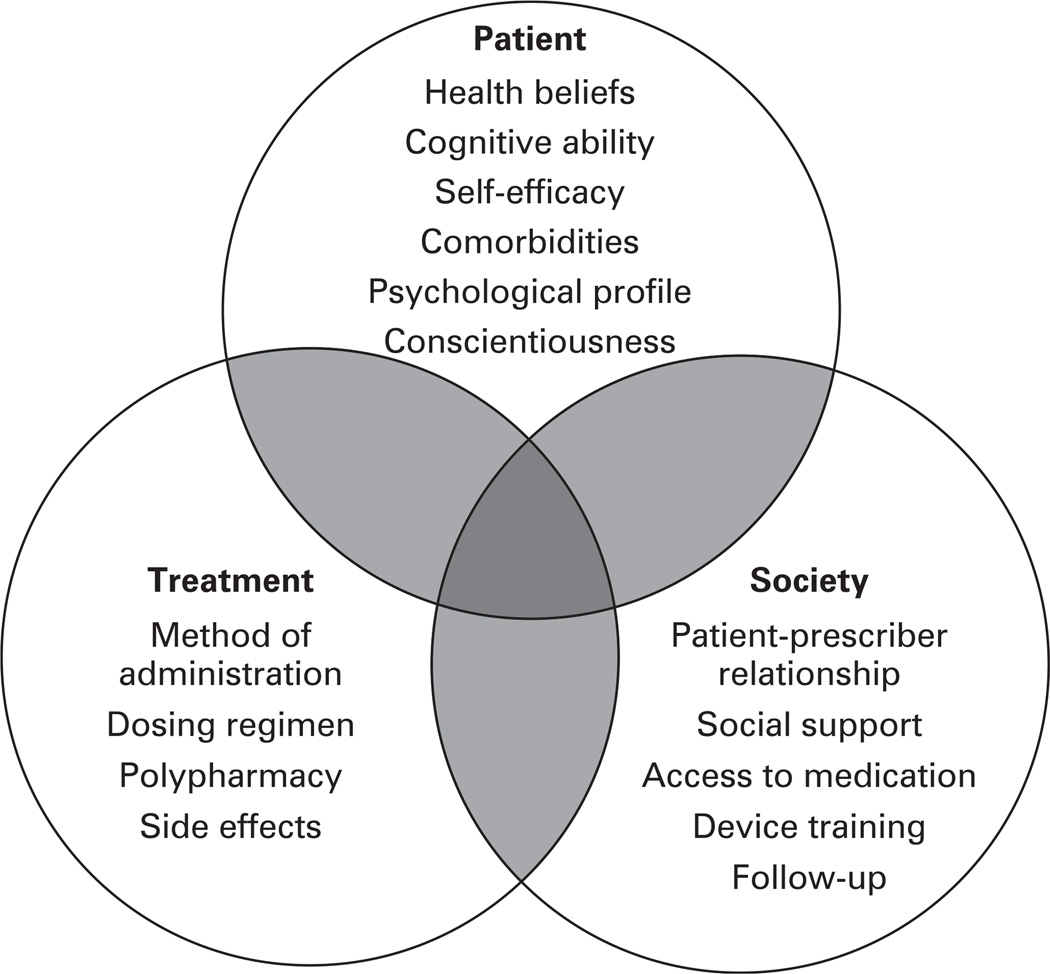
Patient adherence to treatment in chronic obstructive pulmonary disease (COPD) is essential to optimise disease management. As with other chronic diseases, poor adherence is common and results in increased rates of morbidity, healthcare expenditures, hospitalisations and possibly mortality, as well as unnecessary escalation of therapy and reduced quality of life. Examples include overuse, underuse, and alteration of schedule and doses of medication, continued smoking and lack of exercise. Adherence is affected by patients' perception of their disease, type of treatment or medication, the quality of patient provider communication and the social environment. Patients are more likely to adhere to treatment when they believe it will improve disease management or control, or anticipate serious consequences related to non-adherence. Providers play a critical role in helping patients understand the nature of the disease, potential benefits of treatment, addressing concerns regarding potential adverse effects and events, and encouraging patients to develop self-management skills. For clinicians, it is important to explore patients' beliefs and concerns about the safety and benefits of the treatment, as many patients harbour unspoken fears. Complex regimens and polytherapy also contribute to suboptimal adherence. This review addresses adherence related issues in COPD, assesses current efforts to improve adherence and highlights opportunities to improve adherence for both providers and patients.
Figures
Similar articles
-
Impact of patients' perception of COPD and treatment on adherence and health-related quality of life in real-world: Study in 53 community pharmacies.Respir Med. 2021 Jan;176:106280. doi: 10.1016/j.rmed.2020.106280. Epub 2020 Dec 3. Respir Med. 2021. PMID: 33302143
-
Medication adherence issues in patients treated for COPD.Int J Chron Obstruct Pulmon Dis. 2008;3(3):371-84. doi: 10.2147/copd.s3036. Int J Chron Obstruct Pulmon Dis. 2008. PMID: 18990964 Free PMC article. Review.
-
A self-management approach using self-initiated action plans for symptoms with ongoing nurse support in patients with Chronic Obstructive Pulmonary Disease (COPD) and comorbidities: the COPE-III study protocol.Contemp Clin Trials. 2013 Sep;36(1):81-9. doi: 10.1016/j.cct.2013.06.003. Epub 2013 Jun 14. Contemp Clin Trials. 2013. PMID: 23770110 Clinical Trial.
-
[Therapeutic adherence in chronic obstructive pulmonary disease: A literature review].Rev Mal Respir. 2019 Sep;36(7):801-849. doi: 10.1016/j.rmr.2019.06.005. Epub 2019 Jul 9. Rev Mal Respir. 2019. PMID: 31300244 Review. French.
-
Adherence to disease management programs in patients with COPD.Int J Chron Obstruct Pulmon Dis. 2007;2(3):253-62. Int J Chron Obstruct Pulmon Dis. 2007. PMID: 18229563 Free PMC article. Review.
Cited by
-
Practical aspects of inhaler use in the management of chronic obstructive pulmonary disease in the primary care setting.Int J Chron Obstruct Pulmon Dis. 2012;7:495-502. doi: 10.2147/COPD.S32674. Epub 2012 Jul 25. Int J Chron Obstruct Pulmon Dis. 2012. PMID: 22888221 Free PMC article. Review.
-
Inhaled Corticosteroids for Chronic Obstructive Pulmonary Disease--The Shifting Treatment Paradigm.COPD. 2015;12(5):582-90. doi: 10.3109/15412555.2014.995288. Epub 2015 Mar 16. COPD. 2015. PMID: 25774769 Free PMC article. Review.
-
Helping COPD patients change health behavior in order to improve their quality of life.Int J Chron Obstruct Pulmon Dis. 2013;8:335-45. doi: 10.2147/COPD.S34211. Epub 2013 Jul 24. Int J Chron Obstruct Pulmon Dis. 2013. PMID: 23901267 Free PMC article. Review.
-
Patients with underuse or overuse of inhaled corticosteroids have different perceptions and beliefs regarding COPD and inhaled medication.Patient Prefer Adherence. 2018 Sep 12;12:1777-1783. doi: 10.2147/PPA.S167002. eCollection 2018. Patient Prefer Adherence. 2018. PMID: 30254429 Free PMC article.
-
Clinical effectiveness of once-daily fluticasone furoate/umeclidinium/vilanterol in usual practice: the COPD INTREPID study design.ERJ Open Res. 2019 Nov 4;5(4):00061-2019. doi: 10.1183/23120541.00061-2019. eCollection 2019 Oct. ERJ Open Res. 2019. PMID: 31720293 Free PMC article.
References
-
- Halbert RJ, Isonaka S, George D, et al. Interpreting COPD prevalence estimates: what is the true burden of disease? Chest. 2003;123:1684–1692. - PubMed
-
- Murray C, Lopez A. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet. 1997;349:1498–1504. - PubMed
-
- US Department of Health and Human Services NIoHNHLaBI. Chronic obstructive pulmonary disease. [accessed 10 July 2008]; Available at: http://www.nhlbi.nih.gov/health/public/lung/other/copd_fact.htm.
-
- Buist AS, McBurnie MA, Vollmer WM, et al. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370:741–750. - PubMed
-
- Chapman KR, Mannino DM, Soriano JB, et al. Epidemiology and costs of chronic obstructive pulmonary disease. Eur Respir J. 2006;27:188–207. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials