

Characterizing the epidemiological transition in Mexico: national and subnational burden of diseases, injuries, and risk factors
- PMID: 18563960
- PMCID: PMC2429945
- DOI: 10.1371/journal.pmed.0050125
Characterizing the epidemiological transition in Mexico: national and subnational burden of diseases, injuries, and risk factors
Abstract
Background: Rates of diseases and injuries and the effects of their risk factors can have substantial subnational heterogeneity, especially in middle-income countries like Mexico. Subnational analysis of the burden of diseases, injuries, and risk factors can improve characterization of the epidemiological transition and identify policy priorities.
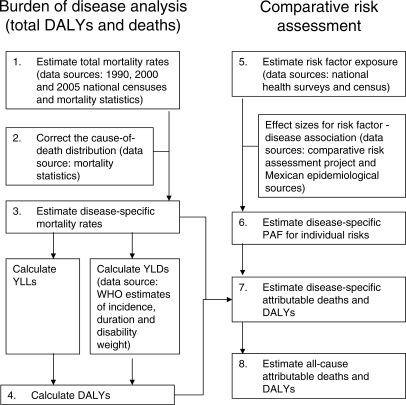
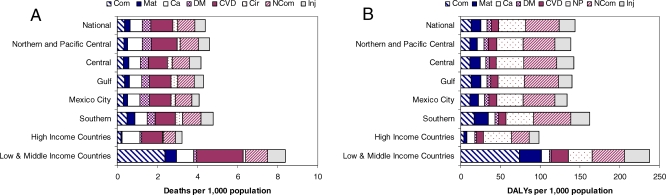
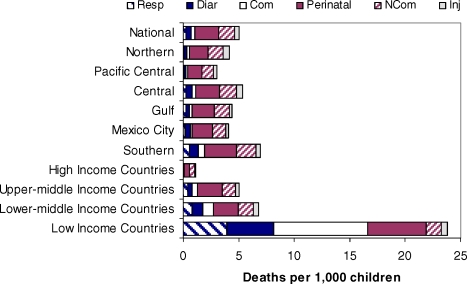
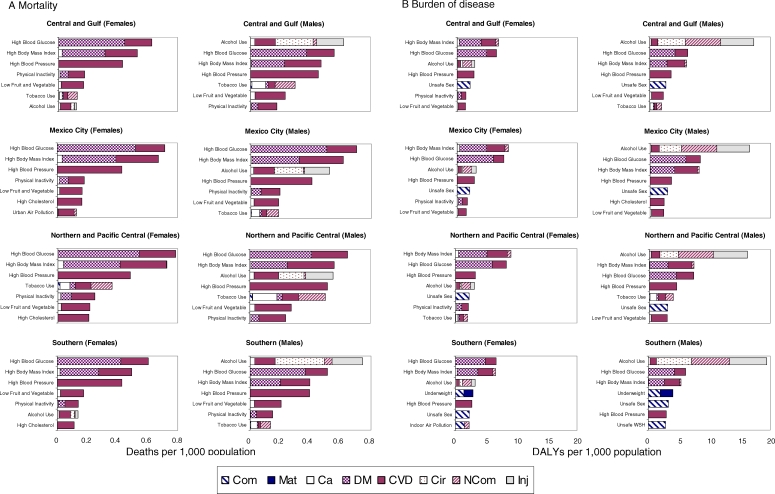
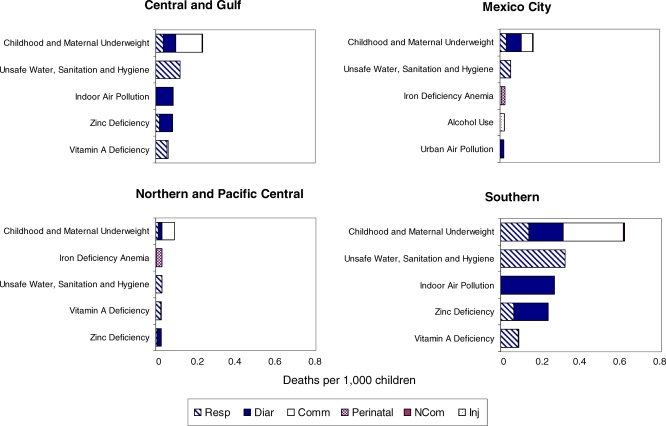
Methods and findings: We estimated deaths and loss of healthy life years (measured in disability-adjusted life years [DALYs]) in 2004 from a comprehensive list of diseases and injuries, and 16 major risk factors, by sex and age for Mexico and its states. Data sources included the vital statistics, national censuses, health examination surveys, and published epidemiological studies. Mortality statistics were adjusted for underreporting, misreporting of age at death, and for misclassification and incomparability of cause-of-death assignment. Nationally, noncommunicable diseases caused 75% of total deaths and 68% of total DALYs, with another 14% of deaths and 18% of DALYs caused by undernutrition and communicable, maternal, and perinatal diseases. The leading causes of death were ischemic heart disease, diabetes mellitus, cerebrovascular disease, liver cirrhosis, and road traffic injuries. High body mass index, high blood glucose, and alcohol use were the leading risk factors for disease burden, causing 5.1%, 5.0%, and 7.3% of total burden of disease, respectively. Mexico City had the lowest mortality rates (4.2 per 1,000) and the Southern region the highest (5.0 per 1,000); under-five mortality in the Southern region was nearly twice that of Mexico City. In the Southern region undernutrition and communicable, maternal, and perinatal diseases caused 23% of DALYs; in Chiapas, they caused 29% of DALYs. At the same time, the absolute rates of noncommunicable disease and injury burdens were highest in the Southern region (105 DALYs per 1,000 population versus 97 nationally for noncommunicable diseases; 22 versus 19 for injuries).
Conclusions: Mexico is at an advanced stage in the epidemiologic transition, with the majority of the disease and injury burden from noncommunicable diseases. A unique characteristic of the epidemiological transition in Mexico is that overweight and obesity, high blood glucose, and alcohol use are responsible for larger burden of disease than other noncommunicable disease risks such as tobacco smoking. The Southern region is least advanced in the epidemiological transition and suffers from the largest burden of ill health in all disease and injury groups.
Conflict of interest statement
Figures
Comment in
-
Subnational burden of disease studies: Mexico leads the way.PLoS Med. 2008 Jun 17;5(6):e138. doi: 10.1371/journal.pmed.0050138. PLoS Med. 2008. PMID: 18563966 Free PMC article.
Similar articles
-
Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study.Lancet. 1997 May 17;349(9063):1436-42. doi: 10.1016/S0140-6736(96)07495-8. Lancet. 1997. PMID: 9164317
-
Dissonant health transition in the states of Mexico, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013.Lancet. 2016 Nov 12;388(10058):2386-2402. doi: 10.1016/S0140-6736(16)31773-1. Epub 2016 Oct 5. Lancet. 2016. PMID: 27720260
-
Mortality by cause for eight regions of the world: Global Burden of Disease Study.Lancet. 1997 May 3;349(9061):1269-76. doi: 10.1016/S0140-6736(96)07493-4. Lancet. 1997. PMID: 9142060
-
The burden of injuries in Mexico: Secondary data analysis from the Global Burden of Disease Study, 1990 to 2019.Injury. 2021 Mar;52(3):467-477. doi: 10.1016/j.injury.2021.02.027. Epub 2021 Feb 15. Injury. 2021. PMID: 33612252 Review.
-
Global burden of disease in young people aged 10-24 years: a systematic analysis.Lancet. 2011 Jun 18;377(9783):2093-102. doi: 10.1016/S0140-6736(11)60512-6. Epub 2011 Jun 7. Lancet. 2011. PMID: 21652063 Review.
Cited by
-
Reclassifying causes of obstetric death in Mexico: a repeated cross-sectional study.Bull World Health Organ. 2016 May 1;94(5):362-369B. doi: 10.2471/BLT.15.163360. Epub 2016 May 2. Bull World Health Organ. 2016. PMID: 27147766 Free PMC article.
-
Does a Reduction in Receiving Assistance With Daily Activities Among Older Adults in Mexico Indicate An Increase in Unmet Needs or a Decrease in Needs for Care?J Gerontol B Psychol Sci Soc Sci. 2024 Apr 1;79(4):gbad192. doi: 10.1093/geronb/gbad192. J Gerontol B Psychol Sci Soc Sci. 2024. PMID: 38142132 Free PMC article.
-
Common values in assessing health outcomes from disease and injury: disability weights measurement study for the Global Burden of Disease Study 2010.Lancet. 2012 Dec 15;380(9859):2129-43. doi: 10.1016/S0140-6736(12)61680-8. Lancet. 2012. PMID: 23245605 Free PMC article.
-
Measuring the population burden of injuries--implications for global and national estimates: a multi-centre prospective UK longitudinal study.PLoS Med. 2011 Dec;8(12):e1001140. doi: 10.1371/journal.pmed.1001140. Epub 2011 Dec 6. PLoS Med. 2011. PMID: 22162954 Free PMC article.
-
Adult mortality attributable to preventable risk factors for non-communicable diseases and injuries in Japan: a comparative risk assessment.PLoS Med. 2012 Jan;9(1):e1001160. doi: 10.1371/journal.pmed.1001160. Epub 2012 Jan 24. PLoS Med. 2012. PMID: 22291576 Free PMC article.
References
-
- Lozano R, Murray CJL, Frenk J, Bobadilla JL. Burden of disease assessment and health system reform: results of a study in Mexico. J Int Dev. 1995;7:555–563.
-
- Murray CJL, Lopez AD. The global burden of disease: a comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020. Boston: Harvard School of Public Health; 1996. 990 p.
-
- Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJL, et al. Selected major risk factors and global and regional burden of disease. Lancet. 2002;360:1347–1360. - PubMed
-
- Mahapatra P. Estimating national burden of disease: the burden of disease in Andhra Pradesh, 1990′s. Hyderabad: Institute of Health Systems; 2002.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
