

Cytomegalovirus-specific T-cell responses and viral replication in kidney transplant recipients
- PMID: 18541023
- PMCID: PMC2432058
- DOI: 10.1186/1479-5876-6-29
Cytomegalovirus-specific T-cell responses and viral replication in kidney transplant recipients
Abstract
Background: Cytomegalovirus (CMV) seronegative recipients (R-) of kidney transplants (KT) from seropositive donors (D+) are at higher risk for CMV replication and ganciclovir(GCV)-resistance than CMV R(+). We hypothesized that low CMV-specific T-cell responses are associated with increased risk of CMV replication in R(+)-patients with D(+) or D(-) donors.
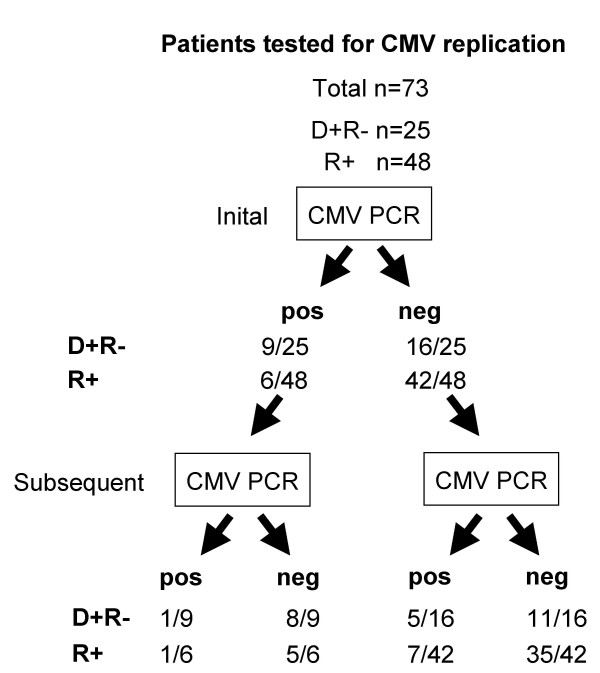
Methods: We prospectively evaluated 73 consecutive KT-patients [48 R(+), 25 D(+)R(-)] undergoing routine testing for CMV replication as part of a preemptive strategy. We compared CMV-specific interferon-gamma (IFN-gamma) responses of CD4+CD3+ lymphocytes in peripheral blood mononuclear cells (PBMC) using three different antigen preparation (CMV-lysate, pp72- and pp65-overlapping peptide pools) using intracellular cytokine staining and flow cytometry.
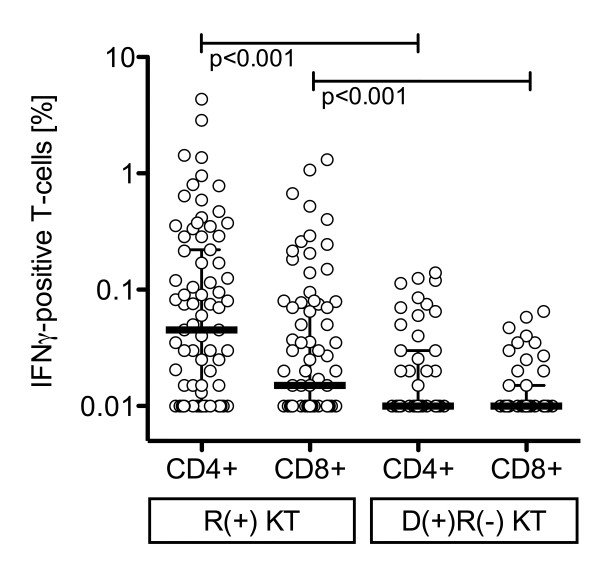
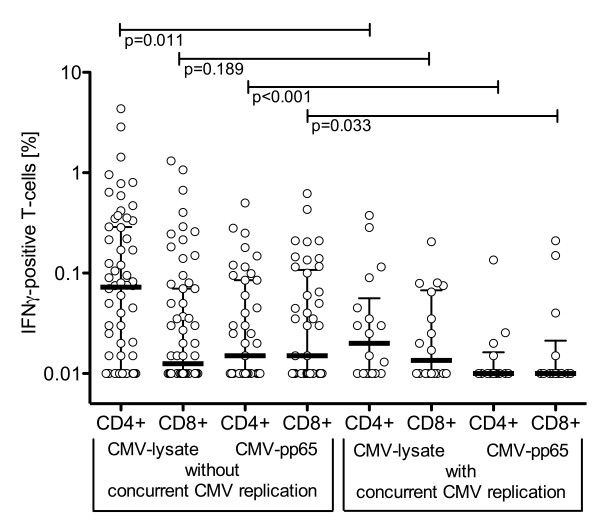
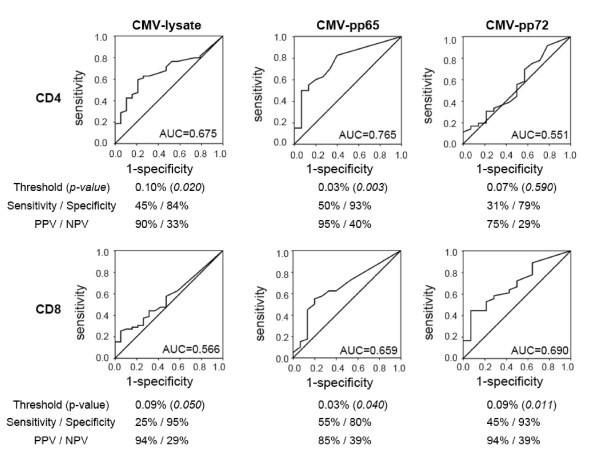
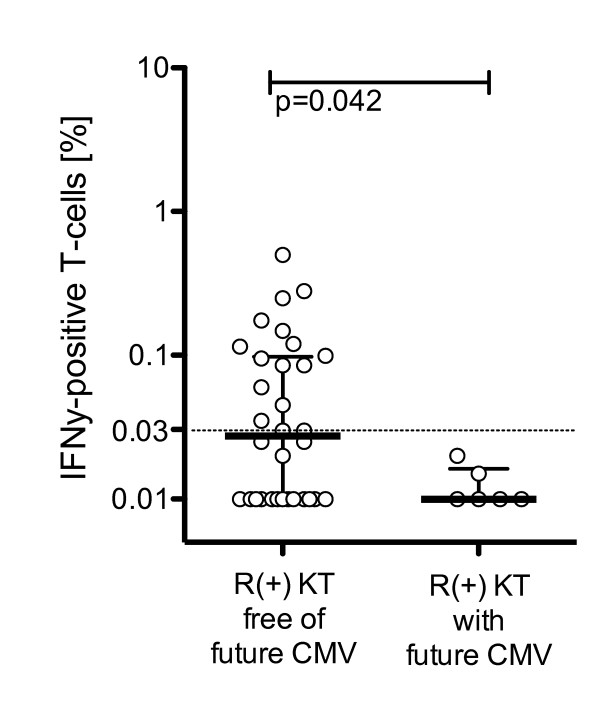
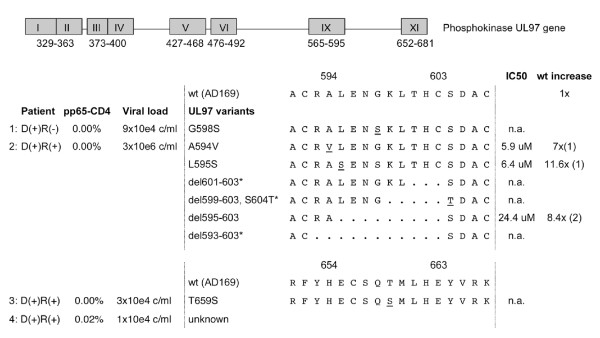
Results: Median CD4+ and CD8+T-cell responses to CMV-lysate, pp72- and pp65-overlapping peptide pools were lower in D(+)R(-) than in R(+)patients or in non-immunosuppressed donors. Comparing subpopulations we found that CMV-lysate favored CD4+- over CD8+-responses, whereas the reverse was observed for pp72, while pp65-CD4+- and -CD8+-responses were similar. Concurrent CMV replication in R(+)-patients was associated with significantly lower T-cell responses (pp65 median CD4+ 0.00% vs. 0.03%, p = 0.001; CD8+ 0.01% vs. 0.03%; p = 0.033). Receiver operated curve analysis associated CMV-pp65 CD4+ responses of > 0.03% in R(+)-patients with absence of concurrent (p = 0.003) and future CMV replication in the following 8 weeks (p = 0.036). GCV-resistant CMV replication occurred in 3 R(+)-patients (6.3%) with pp65- CD4+ frequencies < 0.03% (p = 0.041).
Conclusion: The data suggest that pp65-specific CD4+ T-cells might be useful to identify R(+)-patients at increased risk of CMV replication. Provided further corroborating evidence, CMV-pp65 CD4+ responses above 0.03% in PBMCs of KT patients under stable immunosuppression are associated with lower risk of concurrent and future CMV replication during the following 8 weeks.
Figures
Similar articles
-
[Monitoring of cytomegalovirus-specific CD4+ and CD8+ T cell responses by cytokine flow cytometry in renal transplant recipients].Mikrobiyol Bul. 2016 Apr;50(2):224-35. Mikrobiyol Bul. 2016. PMID: 27175495 Turkish.
-
Regular monitoring of cytomegalovirus-specific cell-mediated immunity in intermediate-risk kidney transplant recipients: predictive value of the immediate post-transplant assessment.Clin Microbiol Infect. 2019 Mar;25(3):381.e1-381.e10. doi: 10.1016/j.cmi.2018.05.010. Epub 2018 May 25. Clin Microbiol Infect. 2019. PMID: 29803844
-
Monitoring cytomegalovirus IE-1 and pp65-specific CD4+ and CD8+ T-cell responses after allogeneic stem cell transplantation may identify patients at risk for recurrent CMV reactivations.Cytometry B Clin Cytom. 2008 Jul;74(4):211-20. doi: 10.1002/cyto.b.20420. Cytometry B Clin Cytom. 2008. PMID: 18454493
-
Cytomegalovirus-associated chorioretinitis after liver transplantation: case report and review of the literature.Transpl Infect Dis. 2008 Feb;10(1):27-43. doi: 10.1111/j.1399-3062.2007.00285.x. Epub 2007 Dec 17. Transpl Infect Dis. 2008. PMID: 18086275 Review.
-
Revisiting the Role of γδ T Cells in Anti-CMV Immune Response after Transplantation.Viruses. 2021 May 29;13(6):1031. doi: 10.3390/v13061031. Viruses. 2021. PMID: 34072610 Free PMC article. Review.
Cited by
-
Clinical factors influencing phenotype of HCMV-specific CD8+ T cells and HCMV-induced interferon-gamma production after allogeneic stem cells transplantation.Clin Dev Immunol. 2013;2013:347213. doi: 10.1155/2013/347213. Epub 2013 Feb 2. Clin Dev Immunol. 2013. PMID: 23424600 Free PMC article.
-
Prospects of Cytomegalovirus-Specific T-Cell Receptors in Clinical Diagnosis and Therapy.Viruses. 2023 Jun 7;15(6):1334. doi: 10.3390/v15061334. Viruses. 2023. PMID: 37376633 Free PMC article. Review.
-
An analysis of regulatory T-cell and Th-17 cell dynamics during cytomegalovirus replication in solid organ transplant recipients.PLoS One. 2012;7(11):e43937. doi: 10.1371/journal.pone.0043937. Epub 2012 Oct 11. PLoS One. 2012. PMID: 23071829 Free PMC article. Clinical Trial.
-
Clinical Experience with Immune Monitoring for Cytomegalovirus in Solid-Organ Transplant Recipients.Curr Infect Dis Rep. 2013 Sep 29. doi: 10.1007/s11908-013-0369-6. Online ahead of print. Curr Infect Dis Rep. 2013. PMID: 24078428
-
Epstein-Barr virus-specific T-cell response in pediatric liver transplant recipients: a cross-sectional study by multiparametric flow cytometry.Front Immunol. 2024 Oct 24;15:1479472. doi: 10.3389/fimmu.2024.1479472. eCollection 2024. Front Immunol. 2024. PMID: 39512353 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
