

Prospective multicenter study of the viral etiology of bronchiolitis in the emergency department
- PMID: 18275439
- PMCID: PMC7187748
- DOI: 10.1111/j.1553-2712.2007.00034.x
Prospective multicenter study of the viral etiology of bronchiolitis in the emergency department
Abstract
Objectives: To determine the viral etiology of bronchiolitis and clinical characteristics of children age < 2 years presenting to the emergency department (ED) with bronchiolitis.
Methods: The authors conducted a 14-center prospective cohort study during 2005-2006 of ED patients age < 2 years with bronchiolitis. The study was conducted in 10 states as part of the Emergency Medicine Network. Researchers collected nasopharyngeal aspirates and conducted structured interviews, medical record reviews, and 2-week follow-up telephone calls. Samples were tested using reverse transcription polymerase chain reaction for respiratory syncytial virus (RSV), rhinovirus (RV), human metapneumovirus (hMPV), and influenza viruses (Flu).
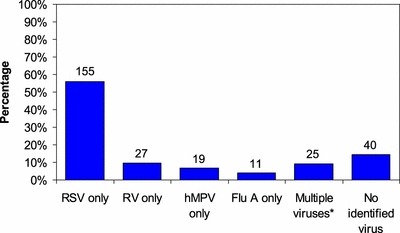
Results: Testing of 277 samples revealed 176 (64%) positive for RSV, 44 (16%) for RV, 26 (9%) for hMPV, 17 (6%) for Flu A, and none for Flu B. When children were categorized as RSV only, RV only, RV and RSV, and all others (hMPV, Flu, no identified virus), children with RV only were more likely to be African American (19, 62, 14, and 40%, respectively; p < 0.001) and have a history of wheezing (23, 52, 21, and 15%, respectively; p = 0.01). In multivariate models, children with RV were more likely to receive corticosteroids (odds ratio [OR] 3.5; 95% confidence interval [CI] = 1.5 to 8.15). The duration of illness may be shorter for children with RV (Days 8, 3, 6, and 8; p = 0.07).
Conclusions: In this multicenter study, RSV was the most frequent cause of bronchiolitis (64%). RV was present in 16%, and these children have a distinct profile in terms of demographics, medical history, and ED treatment.
Figures
Similar articles
-
Detection of new respiratory viruses in hospitalized infants with bronchiolitis: a three-year prospective study.Acta Paediatr. 2010 Jun;99(6):883-7. doi: 10.1111/j.1651-2227.2010.01714.x. Epub 2010 Feb 16. Acta Paediatr. 2010. PMID: 20163373 Free PMC article.
-
[Determination of the frequency of human bocavirus and other respiratory viruses among 0-2 years age group children diagnosed as acute bronchiolitis].Mikrobiyol Bul. 2014 Apr;48(2):242-58. doi: 10.5578/mb.7575. Mikrobiyol Bul. 2014. PMID: 24819262 Turkish.
-
Prospective multicenter study of viral etiology and hospital length of stay in children with severe bronchiolitis.Arch Pediatr Adolesc Med. 2012 Aug;166(8):700-6. doi: 10.1001/archpediatrics.2011.1669. Arch Pediatr Adolesc Med. 2012. PMID: 22473882 Free PMC article.
-
Association of respiratory virus types with clinical features in bronchiolitis: Implications for virus testing strategies. A systematic review and meta-analysis.Paediatr Respir Rev. 2024 Mar;49:34-42. doi: 10.1016/j.prrv.2023.09.003. Epub 2023 Sep 17. Paediatr Respir Rev. 2024. PMID: 37743159 Review.
-
Role of viral infections in the development and exacerbation of asthma in children.J Allergy Clin Immunol. 2017 Oct;140(4):895-906. doi: 10.1016/j.jaci.2017.08.003. J Allergy Clin Immunol. 2017. PMID: 28987219 Free PMC article. Review.
Cited by
-
High incidence of the virus among respiratory pathogens in children with lower respiratory tract infection in northwestern China.J Med Virol. 2023 Jan;95(1):e28367. doi: 10.1002/jmv.28367. J Med Virol. 2023. PMID: 36458544 Free PMC article.
-
Assessing the potential of upper respiratory tract point-of-care testing: a systematic review of the prognostic significance of upper respiratory tract microbes.Clin Microbiol Infect. 2019 Nov;25(11):1339-1346. doi: 10.1016/j.cmi.2019.06.024. Epub 2019 Jun 26. Clin Microbiol Infect. 2019. PMID: 31254715 Free PMC article.
-
In very young infants severity of acute bronchiolitis depends on carried viruses.PLoS One. 2009;4(2):e4596. doi: 10.1371/journal.pone.0004596. Epub 2009 Feb 25. PLoS One. 2009. PMID: 19240806 Free PMC article.
-
Acute respiratory infection emergency access in a tertiary care children hospital in Italy, prior and after the SARS-CoV-2 emergence.Influenza Other Respir Viruses. 2023 Mar 20;17(3):e13102. doi: 10.1111/irv.13102. eCollection 2023 Mar. Influenza Other Respir Viruses. 2023. PMID: 36950039 Free PMC article.
-
Children Hospitalized with Rhinovirus Bronchiolitis Have Asthma-Like Characteristics.J Pediatr. 2016 May;172:202-204.e1. doi: 10.1016/j.jpeds.2016.01.041. Epub 2016 Feb 11. J Pediatr. 2016. PMID: 26875009 Free PMC article.
References
-
- Shay DK, Holman RC, Newman RD, Liu LL, Stout JW, Anderson LJ. Bronchiolitis‐associated hospitalizations among US children, 1980‐1996. JAMA. 1999; 282(15):1440–6. - PubMed
-
- Leader S, Kohlhase K. Respiratory syncytial virus‐coded pediatric hospitalizations, 1997 to 1999. Pediatr Infect Dis J. 2002; 21(7):629–32. - PubMed
-
- Pelletier AJ, Mansbach JM, Camargo CA Jr. Direct medical costs of bronchiolitis hospitalizations in the United States. Pediatrics. 2006; 118(6):2418–23. - PubMed
-
- Papadopoulos NG, Bates PJ, Bardin PG, et al. Rhinoviruses infect the lower airways. J Infect Dis. 2000; 181(6):1875–84. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
