

The healing myocardium sequentially mobilizes two monocyte subsets with divergent and complementary functions
- PMID: 18025128
- PMCID: PMC2118517
- DOI: 10.1084/jem.20070885
The healing myocardium sequentially mobilizes two monocyte subsets with divergent and complementary functions
Abstract
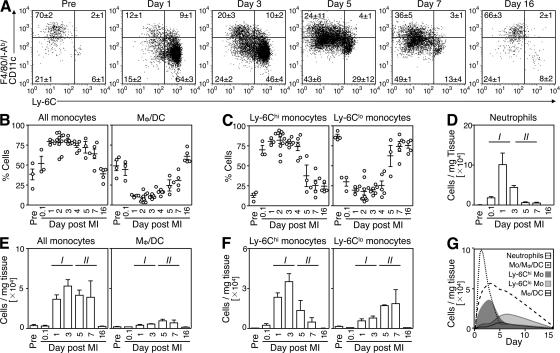
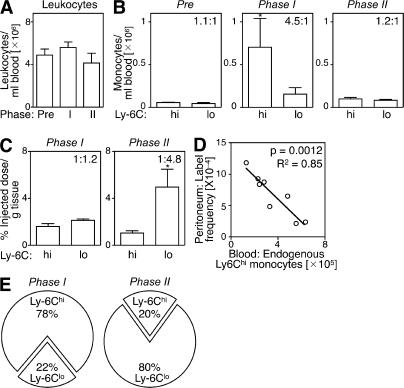
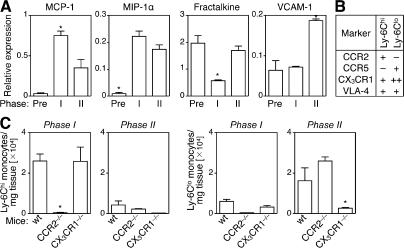
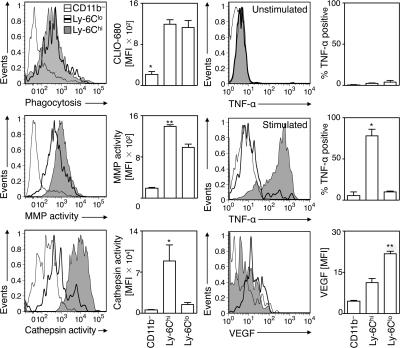
Healing of myocardial infarction (MI) requires monocytes/macrophages. These mononuclear phagocytes likely degrade released macromolecules and aid in scavenging of dead cardiomyocytes, while mediating aspects of granulation tissue formation and remodeling. The mechanisms that orchestrate such divergent functions remain unknown. In view of the heightened appreciation of the heterogeneity of circulating monocytes, we investigated whether distinct monocyte subsets contribute in specific ways to myocardial ischemic injury in mouse MI. We identify two distinct phases of monocyte participation after MI and propose a model that reconciles the divergent properties of these cells in healing. Infarcted hearts modulate their chemokine expression profile over time, and they sequentially and actively recruit Ly-6C(hi) and -6C(lo) monocytes via CCR2 and CX(3)CR1, respectively. Ly-6C(hi) monocytes dominate early (phase I) and exhibit phagocytic, proteolytic, and inflammatory functions. Ly-6C(lo) monocytes dominate later (phase II), have attenuated inflammatory properties, and express vascular-endothelial growth factor. Consequently, Ly-6C(hi) monocytes digest damaged tissue, whereas Ly-6C(lo) monocytes promote healing via myofibroblast accumulation, angiogenesis, and deposition of collagen. MI in atherosclerotic mice with chronic Ly-6C(hi) monocytosis results in impaired healing, underscoring the need for a balanced and coordinated response. These observations provide novel mechanistic insights into the cellular and molecular events that regulate the response to ischemic injury and identify new therapeutic targets that can influence healing and ventricular remodeling after MI.
Figures

Similar articles
-
Impaired infarct healing in atherosclerotic mice with Ly-6C(hi) monocytosis.J Am Coll Cardiol. 2010 Apr 13;55(15):1629-38. doi: 10.1016/j.jacc.2009.08.089. J Am Coll Cardiol. 2010. PMID: 20378083 Free PMC article.
-
Ly-6Chigh monocytes depend on Nr4a1 to balance both inflammatory and reparative phases in the infarcted myocardium.Circ Res. 2014 May 9;114(10):1611-22. doi: 10.1161/CIRCRESAHA.114.303204. Epub 2014 Mar 13. Circ Res. 2014. PMID: 24625784 Free PMC article.
-
Lp-PLA2 Antagonizes Left Ventricular Healing After Myocardial Infarction by Impairing the Appearance of Reparative Macrophages.Circ Heart Fail. 2015 Sep;8(5):980-7. doi: 10.1161/CIRCHEARTFAILURE.115.002334. Epub 2015 Jul 31. Circ Heart Fail. 2015. PMID: 26232205 Free PMC article.
-
Heterogeneous in vivo behavior of monocyte subsets in atherosclerosis.Arterioscler Thromb Vasc Biol. 2009 Oct;29(10):1424-32. doi: 10.1161/ATVBAHA.108.180521. Epub 2009 Apr 16. Arterioscler Thromb Vasc Biol. 2009. PMID: 19372462 Free PMC article. Review.
-
Phagocyte-myocyte interactions and consequences during hypoxic wound healing.Cell Immunol. 2014 Sep-Oct;291(1-2):65-73. doi: 10.1016/j.cellimm.2014.04.006. Epub 2014 May 2. Cell Immunol. 2014. PMID: 24862542 Free PMC article. Review.
Cited by
-
Macrophage plasticity and the role of inflammation in skeletal muscle repair.Mediators Inflamm. 2013;2013:491497. doi: 10.1155/2013/491497. Epub 2013 Jan 30. Mediators Inflamm. 2013. PMID: 23509419 Free PMC article. Review.
-
Eosinophil Deficiency Promotes Aberrant Repair and Adverse Remodeling Following Acute Myocardial Infarction.JACC Basic Transl Sci. 2020 Jul 8;5(7):665-681. doi: 10.1016/j.jacbts.2020.05.005. eCollection 2020 Jul. JACC Basic Transl Sci. 2020. PMID: 32760855 Free PMC article.
-
Enhanced efferocytosis of apoptotic cardiomyocytes through myeloid-epithelial-reproductive tyrosine kinase links acute inflammation resolution to cardiac repair after infarction.Circ Res. 2013 Sep 27;113(8):1004-12. doi: 10.1161/CIRCRESAHA.113.301198. Epub 2013 Jul 8. Circ Res. 2013. PMID: 23836795 Free PMC article.
-
Deleterious Anti-Inflammatory Macrophage Recruitment in Early Post-Infarction Phase: Unraveling the IL-6/MCP-1/STAT3 Axis.JACC Basic Transl Sci. 2024 Apr 24;9(5):593-604. doi: 10.1016/j.jacbts.2024.01.019. eCollection 2024 May. JACC Basic Transl Sci. 2024. PMID: 38984050 Free PMC article.
-
The Immune System in Transfusion-Related Acute Lung Injury Prevention and Therapy: Update and Perspective.Front Mol Biosci. 2021 Mar 24;8:639976. doi: 10.3389/fmolb.2021.639976. eCollection 2021. Front Mol Biosci. 2021. PMID: 33842545 Free PMC article. Review.
References
-
- Sutton, M.G., and N. Sharpe. 2000. Left ventricular remodeling after myocardial infarction: pathophysiology and therapy. Circulation. 101:2981–2988. - PubMed
-
- Blankesteijn, W.M., E. Creemers, E. Lutgens, J.P. Cleutjens, M.J. Daemen, and J.F. Smits. 2001. Dynamics of cardiac wound healing following myocardial infarction: observations in genetically altered mice. Acta Physiol. Scand. 173:75–82. - PubMed
-
- Cleutjens, J.P., W.M. Blankesteijn, M.J. Daemen, and J.F. Smits. 1999. The infarcted myocardium: simply dead tissue, or a lively target for therapeutic interventions. Cardiovasc. Res. 44:232–241. - PubMed
-
- Ertl, G., and S. Frantz. 2005. Healing after myocardial infarction. Cardiovasc. Res. 66:22–32. - PubMed
-
- Frangogiannis, N.G., C.W. Smith, and M.L. Entman. 2002. The inflammatory response in myocardial infarction. Cardiovasc. Res. 53:31–47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
