

Severe human lower respiratory tract illness caused by respiratory syncytial virus and influenza virus is characterized by the absence of pulmonary cytotoxic lymphocyte responses
- PMID: 17357048
- PMCID: PMC7109876
- DOI: 10.1086/512615
Severe human lower respiratory tract illness caused by respiratory syncytial virus and influenza virus is characterized by the absence of pulmonary cytotoxic lymphocyte responses
Abstract
Background: Respiratory syncytial virus (RSV) and influenza virus are common causes of infantile lower respiratory tract infection (LRTI). It is widely believed that both viral replication and inappropriately enhanced immune responses contribute to disease severity. In infants, RSV LRTI is known to be more severe than influenza virus LRTI.
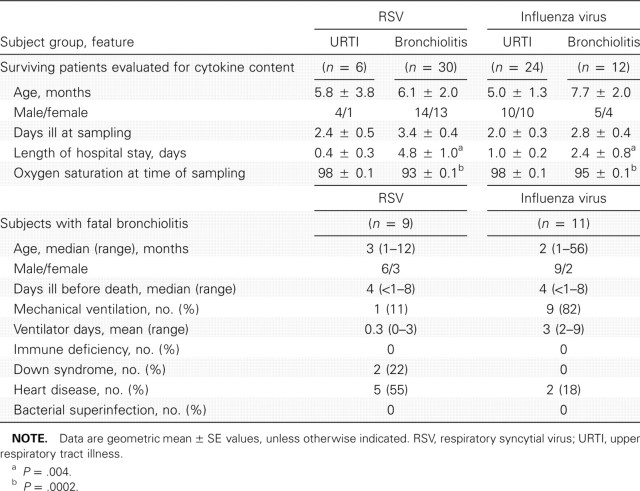
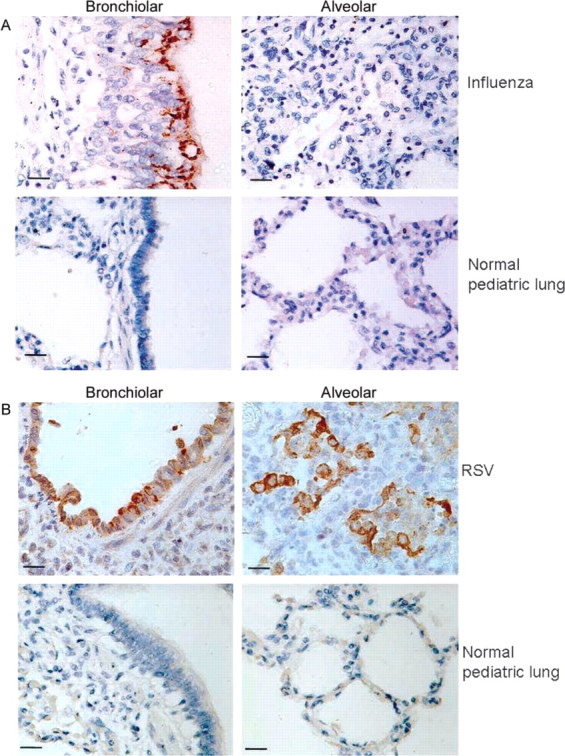
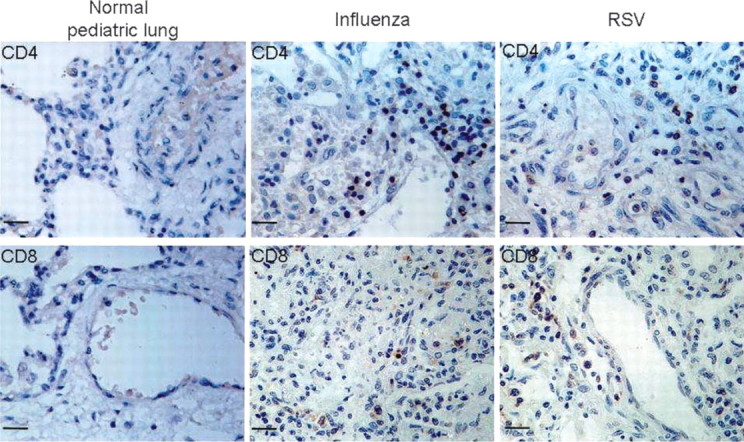
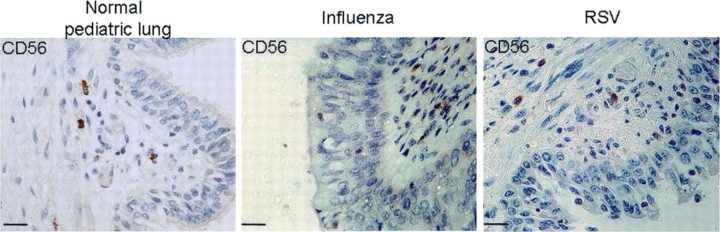
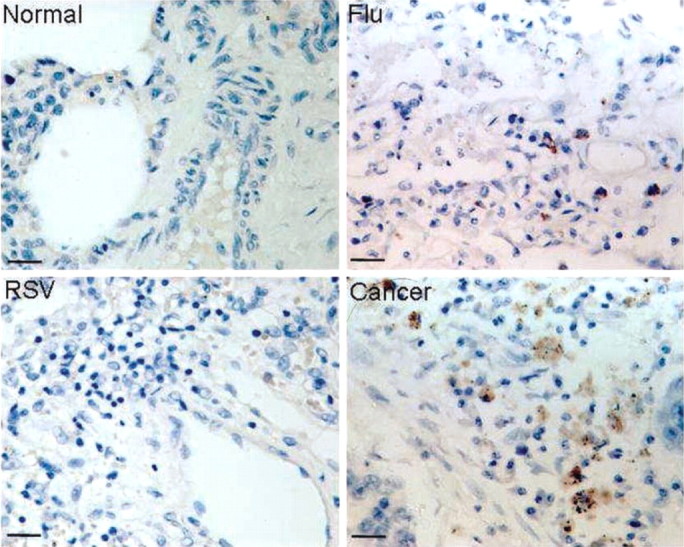
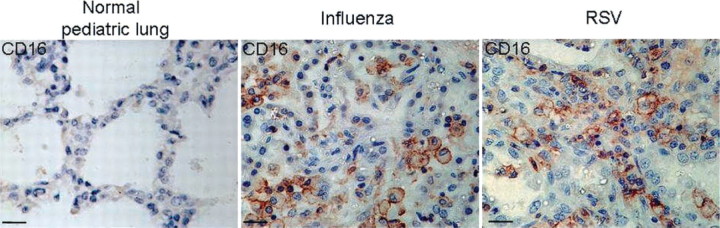
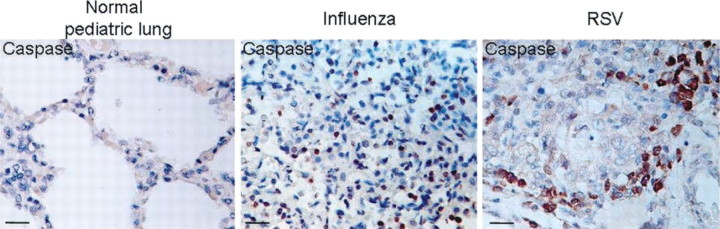
Methods: We compared cytokines and chemokines in secretions of infants surviving various forms of respiratory illness caused by RSV or influenza viruses, to determine which mediators were associated with more-severe illness. We analyzed lung tissue from infants with fatal cases of RSV and influenza virus LRTI to determine the types of inflammatory cells present. Autopsy tissues were studied for the lymphotoxin granzyme and the apoptosis marker caspase 3.
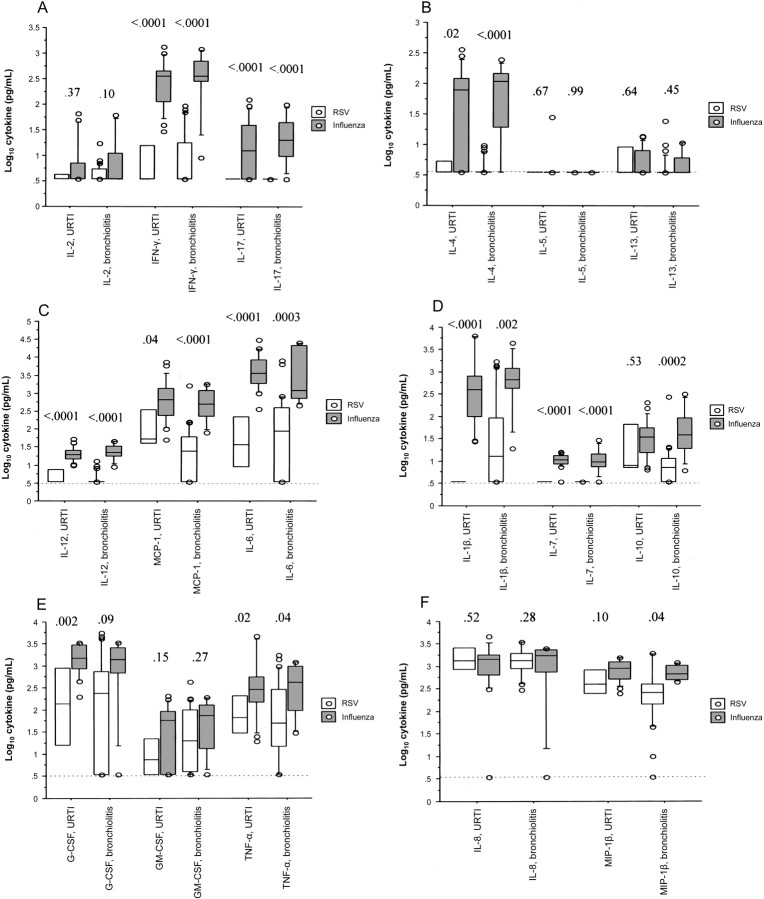
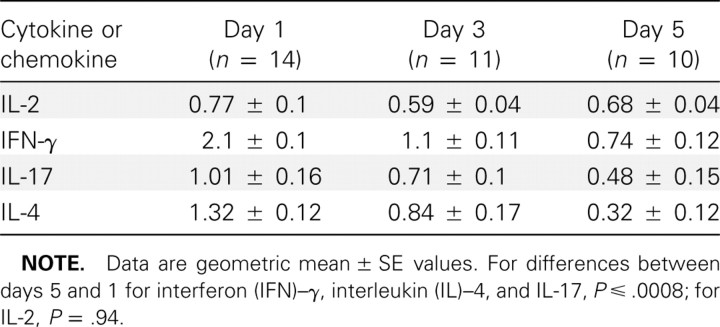
Results: Quantities of lymphocyte-derived cytokines were minimal in secretions from infants with RSV infection. Concentrations of most cytokines were greater in influenza virus, rather than RSV, infection. Lung tissues from infants with fatal RSV and influenza virus LRTI demonstrated an extensive presence of viral antigen and a near absence of CD8-positive lymphocytes and natural killer cells, with marked expression of markers of apoptosis.
Conclusions: Severe infantile RSV and influenza virus LRTI is characterized by inadequate (rather than excessive) adaptive immune responses, robust viral replication, and apoptotic crisis.
Conflict of interest statement
Potential conflicts of interest: none reported.
Figures
Comment in
-
A new direction in understanding the pathogenesis of respiratory syncytial virus bronchiolitis: how real infants suffer.J Infect Dis. 2007 Apr 15;195(8):1084-6. doi: 10.1086/512622. Epub 2007 Mar 9. J Infect Dis. 2007. PMID: 17357042 No abstract available.
Similar articles
-
Respiratory syncytial virus and influenza virus infections: observations from tissues of fatal infant cases.Pediatr Infect Dis J. 2008 Oct;27(10 Suppl):S92-6. doi: 10.1097/INF.0b013e318168b706. Pediatr Infect Dis J. 2008. PMID: 18820587
-
Impaired immune response in severe human lower tract respiratory infection by respiratory syncytial virus.Pediatr Infect Dis J. 2009 Oct;28(10):867-73. doi: 10.1097/INF.0b013e3181a3ea71. Pediatr Infect Dis J. 2009. PMID: 19738511
-
Whole blood gene expression profiles to assess pathogenesis and disease severity in infants with respiratory syncytial virus infection.PLoS Med. 2013 Nov;10(11):e1001549. doi: 10.1371/journal.pmed.1001549. Epub 2013 Nov 12. PLoS Med. 2013. PMID: 24265599 Free PMC article.
-
Mechanisms of illness during respiratory syncytial virus infection: the lungs, the virus and the immune response.Microbes Infect. 2004 Jul;6(8):767-72. doi: 10.1016/j.micinf.2004.03.010. Microbes Infect. 2004. PMID: 15207824 Review.
-
Respiratory syncytial virus in infants: is maternal vaccination a realistic strategy?Curr Opin Infect Dis. 2015 Jun;28(3):221-4. doi: 10.1097/QCO.0000000000000161. Curr Opin Infect Dis. 2015. PMID: 25918956 Review.
Cited by
-
3D engineered tissue models for studying human-specific infectious viral diseases.Bioact Mater. 2022 Sep 22;21:576-594. doi: 10.1016/j.bioactmat.2022.09.010. eCollection 2023 Mar. Bioact Mater. 2022. PMID: 36204281 Free PMC article. Review.
-
Innate Immune Components that Regulate the Pathogenesis and Resolution of hRSV and hMPV Infections.Viruses. 2020 Jun 12;12(6):637. doi: 10.3390/v12060637. Viruses. 2020. PMID: 32545470 Free PMC article. Review.
-
Role of IL-25 in Immunity.J Clin Diagn Res. 2015 Apr;9(4):OE01-4. doi: 10.7860/JCDR/2015/12235.5814. Epub 2015 Apr 1. J Clin Diagn Res. 2015. PMID: 26023586 Free PMC article. Review.
-
Respiratory syncytial virus pathophysiology and affect of palivizumab in special populations: cystic fibrosis and immunosuppression.J Pediatr Pharmacol Ther. 2011 Apr;16(2):74-6. doi: 10.5863/1551-6776-16.2.74. J Pediatr Pharmacol Ther. 2011. PMID: 22477828 Free PMC article. No abstract available.
-
Challenges and opportunities in developing respiratory syncytial virus therapeutics.J Infect Dis. 2015 Mar 15;211 Suppl 1(Suppl 1):S1-S20. doi: 10.1093/infdis/jiu828. J Infect Dis. 2015. PMID: 25713060 Free PMC article.
References
-
- Leader S, Kohlhase K. Respiratory syncytial virus-coded pediatric hospitalizations, 1997 to 1999. Pediatr Infect Dis J. 2002;21:629–32. - PubMed
-
- Garenne M, Ronsmans C, Campbell H. The magnitude of mortality from acute respiratory infections in children under 5 years in developing countries. World Health Stat Q. 1992;45:180–91. - PubMed
-
- Graham BS, Rutigliano JA, Johnson TR. Respiratory syncytial virus immunobiology and pathogenesis. Virology. 2002;297:1–7. - PubMed
-
- McNamara PS, Smyth R. The pathogenesis of respiratory syncytial virus disease in childhood. Brit Med Bull. 2002;61:13–28. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
