

How I treat refractory acute GVHD
- PMID: 17234737
- PMCID: PMC1885485
- DOI: 10.1182/blood-2006-12-041889
How I treat refractory acute GVHD
Abstract
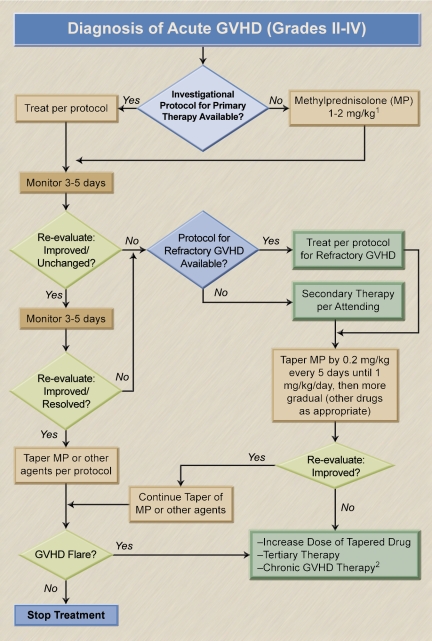
Graft-versus-host disease (GVHD) after allogeneic hematopoietic cell transplantation (HCT) is associated with considerable morbidity and mortality, particularly in patients who do not respond to primary therapy, which usually consists of glucocorticoids (steroids). Approaches to therapy of acute GVHD refractory to "standard" doses of steroids have ranged from increasing the dose of steroids to the addition of polyclonal or monoclonal antibodies, the use of immunotoxins, additional immunosuppressive/chemotherapeutic interventions, phototherapy, and other means. While many pilot studies have yielded encouraging response rates, in most of these studies long-term survival was not improved in comparison with that seen with the use of steroids alone. A major reason for failure has been the high rate of infections, including invasive fungal, bacterial, and viral infections. It is difficult to conduct controlled prospective trials in the setting of steroid-refractory GVHD, and a custom-tailored therapy dependent upon the time after HCT, specific organ manifestations of GVHD, and severity is appropriate. All patients being treated for GVHD should also receive intensive prophylaxis against infectious complications.
Figures
Similar articles
-
The Potential of Mesenchymal Stromal Cells as Treatment for Severe Steroid-Refractory Acute Graft-Versus-Host Disease: A Critical Review of the Literature.Transplantation. 2016 Nov;100(11):2309-2314. doi: 10.1097/TP.0000000000001029. Transplantation. 2016. PMID: 26714122 Review.
-
Pharmaceutical and cellular strategies in prophylaxis and treatment of graft-versus-host disease.Curr Pharm Des. 2009;15(17):1974-97. doi: 10.2174/138161209788453158. Curr Pharm Des. 2009. PMID: 19519437 Review.
-
Acute graft-vs-host disease: pathobiology and management.Exp Hematol. 2001 Mar;29(3):259-77. doi: 10.1016/s0301-472x(00)00677-9. Exp Hematol. 2001. PMID: 11274753 Review.
-
Alloreactivity as therapeutic principle in the treatment of hematologic malignancies. Studies of clinical and immunologic aspects of allogeneic hematopoietic cell transplantation with nonmyeloablative conditioning.Dan Med Bull. 2007 May;54(2):112-39. Dan Med Bull. 2007. PMID: 17521527 Review.
-
New therapeutic targets and biomarkers for acute graft-versus-host disease (GVHD).Expert Opin Ther Targets. 2021 Sep;25(9):761-771. doi: 10.1080/14728222.2021.1992383. Epub 2021 Nov 1. Expert Opin Ther Targets. 2021. PMID: 34669521 Free PMC article. Review.
Cited by
-
Use of mesenchymal stem cells (MSC) in chronic inflammatory fistulizing and fibrotic diseases: a comprehensive review.Clin Rev Allergy Immunol. 2013 Oct;45(2):180-92. doi: 10.1007/s12016-012-8347-6. Clin Rev Allergy Immunol. 2013. PMID: 23296948 Review.
-
DLL4+ dendritic cells: Key regulators of Notch Signaling in effector T cell responses.Pharmacol Res. 2016 Nov;113(Pt A):449-457. doi: 10.1016/j.phrs.2016.09.001. Epub 2016 Sep 14. Pharmacol Res. 2016. PMID: 27639599 Free PMC article. Review.
-
Applications of PET in Diagnosis and Prognosis of Leukemia.Technol Cancer Res Treat. 2020 Jan-Dec;19:1533033820956993. doi: 10.1177/1533033820956993. Technol Cancer Res Treat. 2020. PMID: 32875963 Free PMC article. Review.
-
Atorvastatin for the Prophylaxis of Acute Graft-versus-Host Disease in Patients Undergoing HLA-Matched Related Donor Allogeneic Hematopoietic Stem Cell Transplantation (allo-HCT).Biol Blood Marrow Transplant. 2016 Jan;22(1):71-9. doi: 10.1016/j.bbmt.2015.07.034. Epub 2015 Aug 6. Biol Blood Marrow Transplant. 2016. PMID: 26256940 Free PMC article. Clinical Trial.
-
A 16 Month Survey of Cyclosporine Utilization Evaluation in Allogeneic Hematopoietic Stem Cell Transplant Recipients.Iran J Pharm Res. 2016 Winter;15(1):331-9. Iran J Pharm Res. 2016. PMID: 27610174 Free PMC article.
References
-
- Lorenz E, Uphoff D, Reid TR, Shelton E. Modification of irradiation injury in mice and guinea pigs by bone marrow injections. J Natl Cancer Inst. 1951;12:197–201. - PubMed
-
- van Bekkum DW, de Vries MJ. Radiation Chimaeras. London, United Kingdom: Logos Press Limited; 1967. The production of radiation chimaeras. pp. 20–78.
-
- Billingham RE. The Harvey Lectures. New York, NY: Academic Press; 1966. The biology of graft-versus-host reactions; pp. 21–78. - PubMed
-
- Ferrara JLM, Cooke KR, Deeg HJ, editors. 3rd ed. New York, NY: Marcel Dekker; 2005. Graft-vs.-Host Disease.
-
- Shlomchik WD, Couzens MS, Tang CB, et al. Prevention of graft versus host disease by inactivation of host antigen-presenting cells. Science. 1999;285:412–415. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
