

A prospective, randomized, controlled trial comparing intermittent portal triad clamping versus ischemic preconditioning with continuous clamping for major liver resection
- PMID: 17122617
- PMCID: PMC1856627
- DOI: 10.1097/01.sla.0000246834.07130.5d
A prospective, randomized, controlled trial comparing intermittent portal triad clamping versus ischemic preconditioning with continuous clamping for major liver resection
Abstract
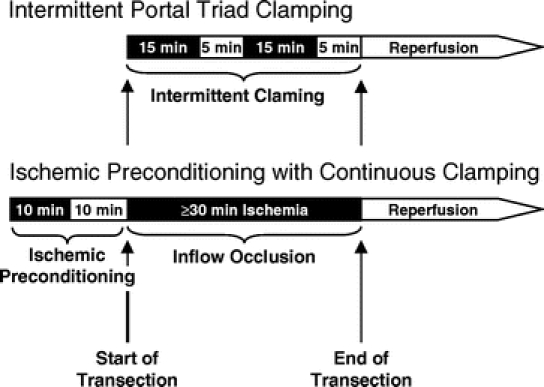
Objective: To evaluate whether ischemic preconditioning (IP) with continuous clamping or intermittent clamping (IC) of the portal triad confers better protection during liver surgery.
Summary background data: IP and IC are distinct protective approaches against ischemic injury. Since both strategies proved to be superior in randomized controlled trials (RCTs) to continuous inflow occlusion alone, we designed a RCT to compare IP and IC in patients undergoing major liver resection.
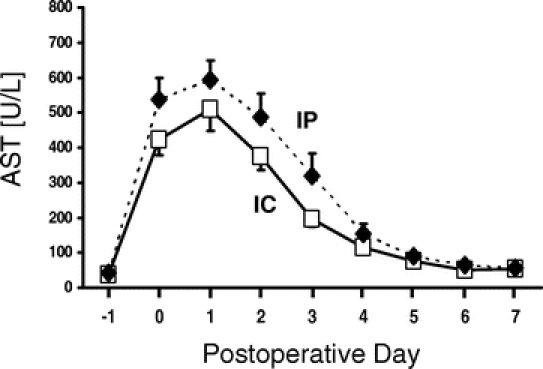
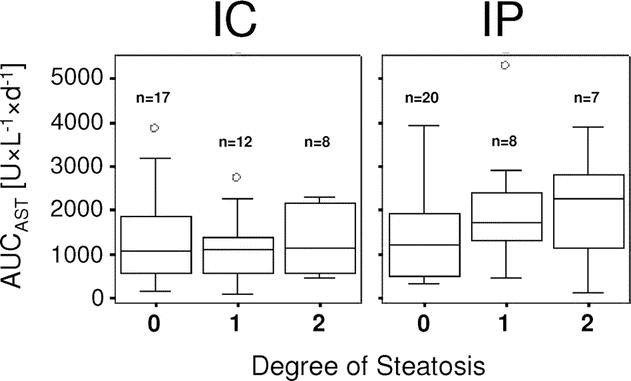
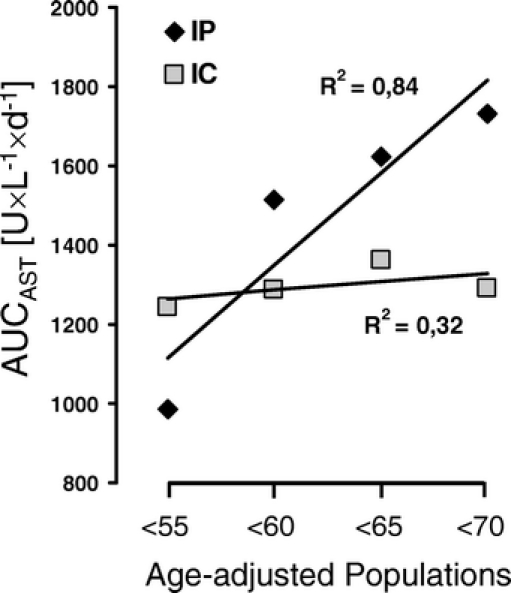
Methods: Noncirrhotic patients undergoing major liver resection were randomized to receive IP with inflow occlusion (n = 36) or IC (n = 37). Primary endpoints were postoperative liver injury and intraoperative blood loss. Postoperative liver injury was assessed by peak values of AST (alanine aminotransferase) and ALT (aspartate aminotransferase), as well as the area under the curve (AUC) of the postoperative transaminase course. Secondary endpoints included resection time, the need of blood transfusion, ICU, and hospital stay as well as postoperative complications and mortality.
Results: Both groups were comparable regarding demographics, ASA score, type of hepatectomy, duration of inflow occlusion (range, 30-75 minutes), and resection surface. The transection-related blood loss was 146 versus 250 mL (P = 0.008), and when standardized to the resection surface 1.2 versus 1.8 mL/cm (P = 0.01) for IP and IC, respectively. Although peak AST, AUCAST, and AUCALT were lower for IC, the differences did not reach statistical significance. Overall (42% vs. 38%) and major (33 vs. 27%) postoperative complications as well as median ICU (1 vs. 1 day) and hospital stay (10 vs. 11 days) were similar between both groups.
Conclusions: Both IP and IC appear to be equally effective in protecting against postoperative liver injury in noncirrhotic patients undergoing major liver resection. However, IP is associated with lower blood loss and shorter transection time. Therefore, both strategies can be recommended for noncirrhotic patients undergoing liver resection.
Figures
Similar articles
-
Methods of vascular occlusion for elective liver resections.Cochrane Database Syst Rev. 2007 Oct 17;(4):CD006409. doi: 10.1002/14651858.CD006409.pub2. Cochrane Database Syst Rev. 2007. Update in: Cochrane Database Syst Rev. 2009 Jan 21;(1):CD006409. doi: 10.1002/14651858.CD006409.pub3 PMID: 17943908 Updated. Review.
-
WITHDRAWN: Methods of vascular occlusion for elective liver resections.Cochrane Database Syst Rev. 2009 Jan 21;2009(1):CD006409. doi: 10.1002/14651858.CD006409.pub3. Cochrane Database Syst Rev. 2009. PMID: 19160283 Free PMC article. Review.
-
Randomized clinical trial of ischaemic preconditioning in major liver resection with intermittent Pringle manoeuvre.Br J Surg. 2011 Sep;98(9):1236-43. doi: 10.1002/bjs.7626. Epub 2011 Jul 11. Br J Surg. 2011. PMID: 21809337 Clinical Trial.
-
Ischemic preconditioning improves postoperative outcome after liver resections: a randomized controlled study.Eur J Med Res. 2008 Feb 25;13(2):79-86. Eur J Med Res. 2008. PMID: 18424367 Clinical Trial.
-
Ischemic preconditioning provides no additive clinical value in liver resection of cirrhotic and non-cirrhotic patients under portal triad clamping: a prospective randomized controlled trial.Clin Res Hepatol Gastroenterol. 2014 Sep;38(4):467-74. doi: 10.1016/j.clinre.2014.03.013. Epub 2014 Apr 29. Clin Res Hepatol Gastroenterol. 2014. PMID: 24787266 Clinical Trial.
Cited by
-
Intermittent clamping is superior to ischemic preconditioning and its effect is more marked with shorter clamping cycles in the rat liver.J Gastroenterol. 2013 Jan;48(1):115-24. doi: 10.1007/s00535-012-0613-0. Epub 2012 Jun 16. J Gastroenterol. 2013. PMID: 22706572
-
Red blood cell transfusion in liver resection.Langenbecks Arch Surg. 2019 Feb;404(1):1-9. doi: 10.1007/s00423-018-1746-2. Epub 2019 Jan 3. Langenbecks Arch Surg. 2019. PMID: 30607533 Review.
-
Hydrogen sulfide preconditioning protects rat liver against ischemia/reperfusion injury by activating Akt-GSK-3β signaling and inhibiting mitochondrial permeability transition.PLoS One. 2013 Sep 13;8(9):e74422. doi: 10.1371/journal.pone.0074422. eCollection 2013. PLoS One. 2013. PMID: 24058562 Free PMC article.
-
Ischemic preconditioning confers antiapoptotic protection during major hepatectomies performed under combined inflow and outflow exclusion of the liver. A randomized clinical trial.World J Surg. 2009 Sep;33(9):1909-15. doi: 10.1007/s00268-009-0117-0. World J Surg. 2009. PMID: 19575143 Clinical Trial.
-
Efficacy of high-intensity focused ultrasound-assisted hepatic resection (HIFU-AR) on blood loss reduction in patients with liver metastases requiring hepatectomy: study protocol for a randomized controlled trial.Trials. 2017 Feb 6;18(1):57. doi: 10.1186/s13063-017-1801-2. Trials. 2017. PMID: 28166812 Free PMC article. Clinical Trial.
References
-
- Belghiti J, Hiramatsu K, Benoist S, et al. Seven hundred forty-seven hepatectomies in the 1990s: an update to evaluate the actual risk of liver resection. J Am Coll Surg. 2000;191:38–46. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
