

The mechanism of diabetes control after gastrointestinal bypass surgery reveals a role of the proximal small intestine in the pathophysiology of type 2 diabetes
- PMID: 17060767
- PMCID: PMC1856597
- DOI: 10.1097/01.sla.0000224726.61448.1b
The mechanism of diabetes control after gastrointestinal bypass surgery reveals a role of the proximal small intestine in the pathophysiology of type 2 diabetes
Abstract
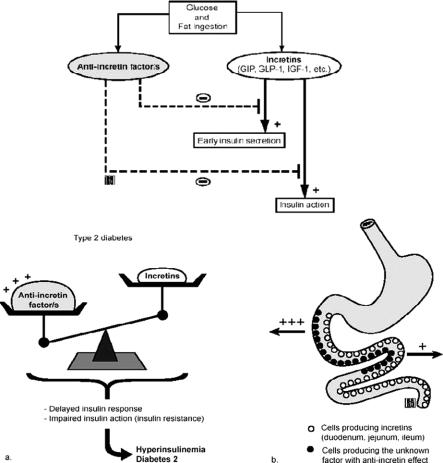
Summary background data: Most patients who undergo Roux-en-Y gastric bypass (RYGB) experience rapid resolution of type 2 diabetes. Prior studies indicate that this results from more than gastric restriction and weight loss, implicating the rearranged intestine as a primary mediator. It is unclear, however, if diabetes improves because of enhanced delivery of nutrients to the distal intestine and increased secretion of hindgut signals that improve glucose homeostasis, or because of altered signals from the excluded segment of proximal intestine. We sought to distinguish between these two mechanisms.
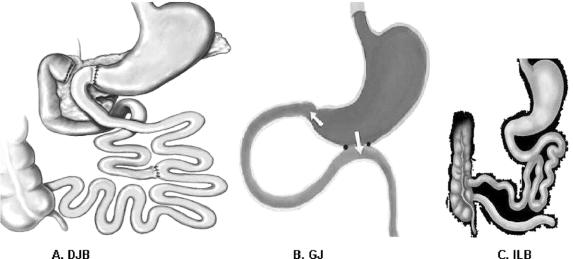
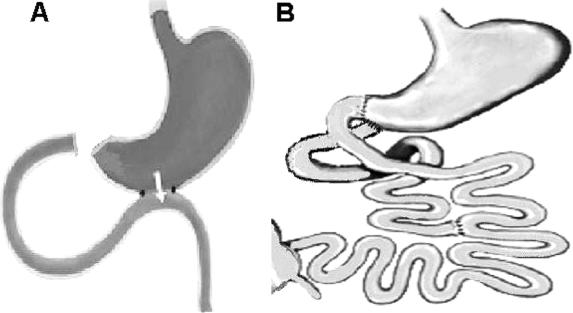
Methods: Goto-Kakizaki (GK) type 2 diabetic rats underwent duodenal-jejunal bypass (DJB), a stomach-preserving RYGB that excludes the proximal intestine, or a gastrojejunostomy (GJ), which creates a shortcut for ingested nutrients without bypassing any intestine. Controls were pair-fed (PF) sham-operated and untreated GK rats. Rats that had undergone GJ were then reoperated to exclude the proximal intestine; and conversely, duodenal passage was restored in rats that had undergone DJB. Oral glucose tolerance (OGTT), food intake, body weight, and intestinal nutrient absorption were measured.
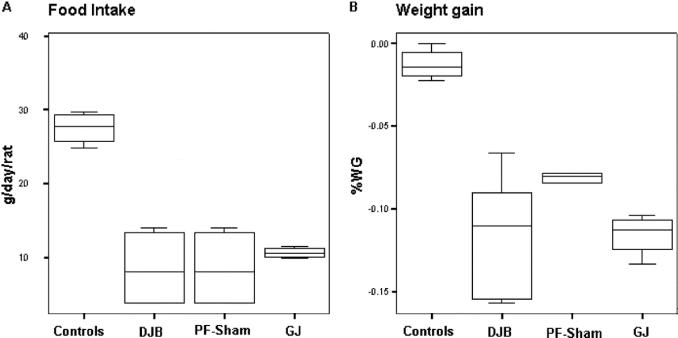
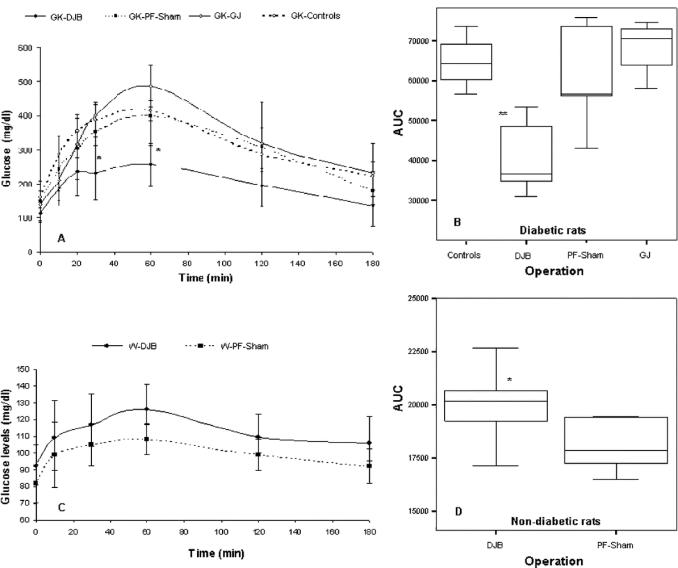
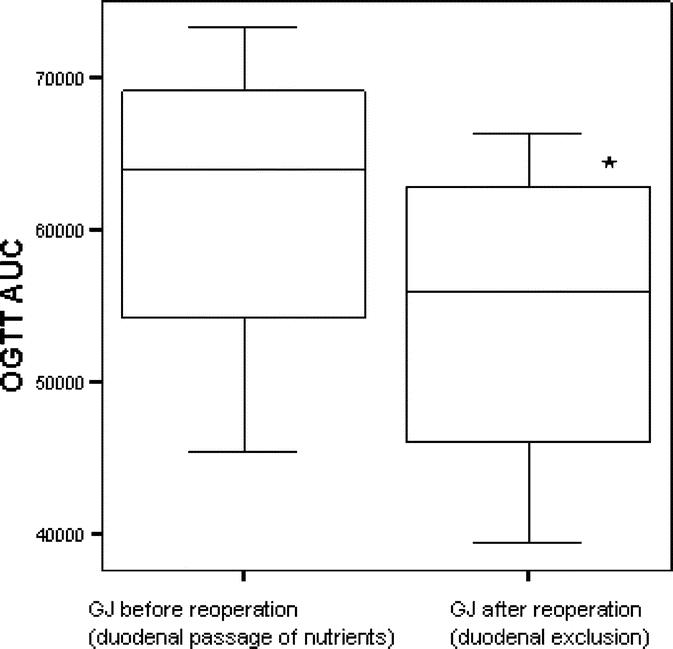
Results: There were no differences in food intake, body weight, or nutrient absorption among surgical groups. DJB-treated rats had markedly better oral glucose tolerance compared with all control groups as shown by lower peak and area-under-the-curve glucose values (P < 0.001 for both). GJ did not affect glucose homeostasis, but exclusion of duodenal nutrient passage in reoperated GJ rats significantly improved glucose tolerance. Conversely, restoration of duodenal passage in DJB rats reestablished impaired glucose tolerance.
Conclusions: This study shows that bypassing a short segment of proximal intestine directly ameliorates type 2 diabetes, independently of effects on food intake, body weight, malabsorption, or nutrient delivery to the hindgut. These findings suggest that a proximal intestinal bypass could be considered for diabetes treatment and that potentially undiscovered factors from the proximal bowel might contribute to the pathophysiology of type 2 diabetes.
Figures
Similar articles
-
[Effect of blood glucose control after small intestine exclusion surgery in Goto-Kakizaki rat with type 2 diabetes mellitus].Zhonghua Yi Xue Za Zhi. 2009 Nov 3;89(40):2858-61. Zhonghua Yi Xue Za Zhi. 2009. PMID: 20137669 Chinese.
-
The Effect of Gastric Bypass with a Distal Gastric Pouch on Glucose Tolerance and Diabetes Remission in Type 2 Diabetes Sprague-Dawley Rat Model.Obes Surg. 2019 Jun;29(6):1889-1900. doi: 10.1007/s11695-019-03776-w. Obes Surg. 2019. PMID: 30778846
-
Roux-en Y gastric bypass is superior to duodeno-jejunal bypass in improving glycaemic control in Zucker diabetic fatty rats.Obes Surg. 2014 Nov;24(11):1888-95. doi: 10.1007/s11695-014-1301-3. Obes Surg. 2014. PMID: 24927690
-
Neuro-modulation and bariatric surgery for type 2 diabetes mellitus.Int J Clin Pract Suppl. 2010 Feb;(166):53-8. doi: 10.1111/j.1742-1241.2009.02279.x. Int J Clin Pract Suppl. 2010. PMID: 20377665 Review.
-
Mechanisms of early improvement/resolution of type 2 diabetes after bariatric surgery.Diabetes Metab. 2009 Dec;35(6 Pt 2):518-23. doi: 10.1016/S1262-3636(09)73459-7. Diabetes Metab. 2009. PMID: 20152737 Review.
Cited by
-
Surgical treatment of type 2 diabetes in patients with BMI below 35: mid-term outcomes of the laparoscopic ileal interposition associated with a sleeve gastrectomy in 202 consecutive cases.J Gastrointest Surg. 2012 May;16(5):967-76. doi: 10.1007/s11605-011-1807-0. Epub 2012 Feb 18. J Gastrointest Surg. 2012. PMID: 22350720
-
Mechanisms behind the immediate effects of Roux-en-Y gastric bypass surgery on type 2 diabetes.Theor Biol Med Model. 2013 Jul 13;10:45. doi: 10.1186/1742-4682-10-45. Theor Biol Med Model. 2013. PMID: 23849268 Free PMC article.
-
Myocardial insulin signaling and glucose transport are up-regulated in Goto-Kakizaki type 2 diabetic rats after ileal transposition.Obes Surg. 2012 Mar;22(3):493-501. doi: 10.1007/s11695-012-0604-5. Obes Surg. 2012. PMID: 22249887
-
C-peptide predicts the remission of type 2 diabetes after bariatric surgery.Obes Surg. 2012 Feb;22(2):293-8. doi: 10.1007/s11695-011-0565-0. Obes Surg. 2012. PMID: 22139820
-
Correlation between body mass index and gut concentrations of Lactobacillus reuteri, Bifidobacterium animalis, Methanobrevibacter smithii and Escherichia coli.Int J Obes (Lond). 2013 Nov;37(11):1460-6. doi: 10.1038/ijo.2013.20. Epub 2013 Mar 5. Int J Obes (Lond). 2013. Retraction in: Int J Obes (Lond). 2024 Sep;48(9):1356. doi: 10.1038/s41366-024-01557-9. PMID: 23459324 Free PMC article. Retracted.
References
-
- Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004 13;292:1724–1737. - PubMed
-
- Sjostrom L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683–2693. - PubMed
-
- Cummings DE, Overduin J, Foster-Schubert KE. Gastric bypass for obesity: mechanisms of weight loss and diabetes resolution. J Clin Endocrinol Metab. 2004;89:2608–2615. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
