

Checkpoint blockade in cancer immunotherapy
- PMID: 16730267
- PMCID: PMC1951510
- DOI: 10.1016/S0065-2776(06)90008-X
Checkpoint blockade in cancer immunotherapy
Abstract
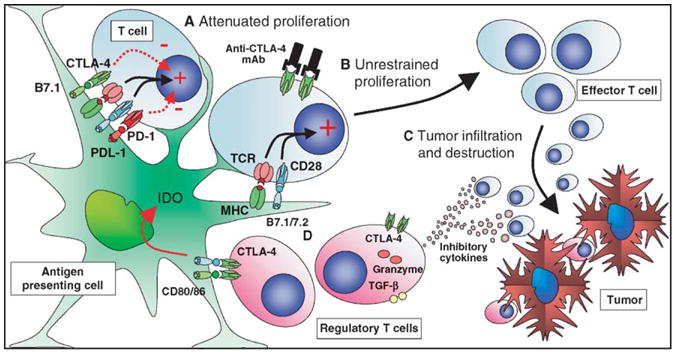
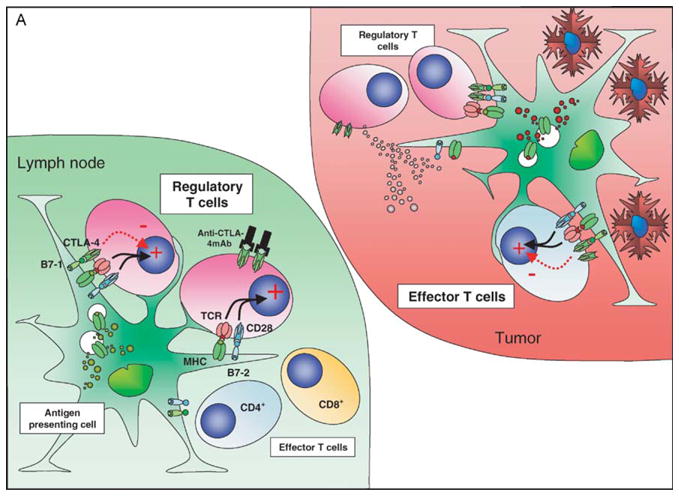
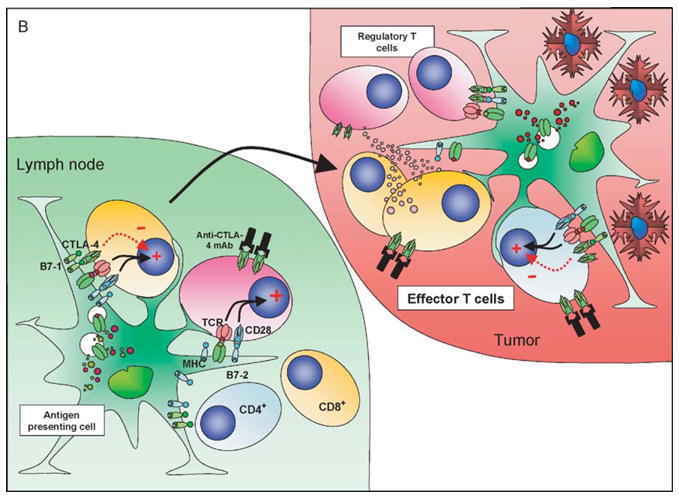
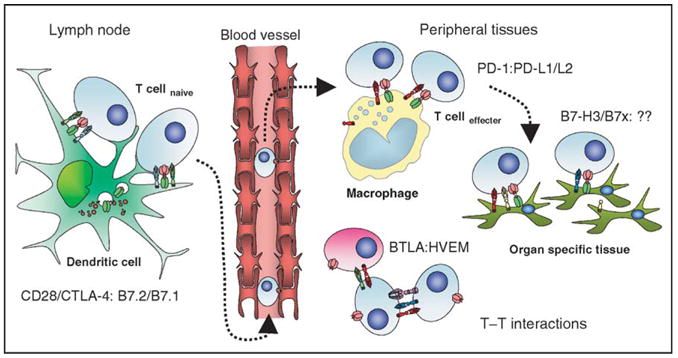
The progression of a productive immune response requires that a number of immunological checkpoints be passed. Passage may require the presence of excitatory costimulatory signals or the avoidance of negative or coinhibitory signals, which act to dampen or terminate immune activity. The immunoglobulin superfamily occupies a central importance in this coordination of immune responses, and the CD28/cytotoxic T-lymphocyte antigen-4 (CTLA-4):B7.1/B7.2 receptor/ligand grouping represents the archetypal example of these immune regulators. In part the role of these checkpoints is to guard against the possibility of unwanted and harmful self-directed activities. While this is a necessary function, aiding in the prevention of autoimmunity, it may act as a barrier to successful immunotherapies aimed at targeting malignant self-cells that largely display the same array of surface molecules as the cells from which they derive. Therapies aimed at overcoming these mechanisms of peripheral tolerance, in particular by blocking the inhibitory checkpoints, offer the potential to generate antitumor activity, either as monotherapies or in synergism with other therapies that directly or indirectly enhance presentation of tumor epitopes to the immune system. Such immunological molecular adjuvants are showing promise in early clinical trials. This review focuses on the results of the archetypal example of checkpoint blockade, anti-CTLA-4, in preclinical tumor models and clinical trials, while also highlighting other possible targets for immunological checkpoint blockade.
Figures
Similar articles
-
Cell intrinsic mechanisms of T-cell inhibition and application to cancer therapy.Immunol Rev. 2008 Aug;224:141-65. doi: 10.1111/j.1600-065X.2008.00649.x. Immunol Rev. 2008. PMID: 18759925 Review.
-
Immune checkpoint therapy for non-small-cell lung cancer: an update.Immunotherapy. 2016;8(3):279-98. doi: 10.2217/imt.15.123. Epub 2016 Feb 9. Immunotherapy. 2016. PMID: 26860624 Review.
-
Nobel goes to immune checkpoint-Innovative cancer treatment by immunotherapy.Sci China Life Sci. 2018 Nov;61(11):1445-1450. doi: 10.1007/s11427-018-9409-7. Epub 2018 Oct 29. Sci China Life Sci. 2018. PMID: 30377902 No abstract available.
-
Activity and safety of CTLA-4 blockade combined with vaccines in cynomolgus macaques.J Immunol. 2003 Dec 1;171(11):6251-9. doi: 10.4049/jimmunol.171.11.6251. J Immunol. 2003. PMID: 14634142
-
CTLA-4: negative regulator of the immune response and a target for cancer therapy.J Immunother. 2008 Jun;31(5):431-9. doi: 10.1097/CJI.0b013e318174a4fe. J Immunother. 2008. PMID: 18463542 Review.
Cited by
-
Dendritic cells transfected with a polyepitope DNA construct stimulate an antitumor cytotoxic response in various tumors.Mol Clin Oncol. 2022 Oct 3;17(5):155. doi: 10.3892/mco.2022.2588. eCollection 2022 Nov. Mol Clin Oncol. 2022. PMID: 36325297 Free PMC article.
-
TLR2/6 agonists and interferon-gamma induce human melanoma cells to produce CXCL10.Int J Cancer. 2015 Sep 15;137(6):1386-96. doi: 10.1002/ijc.29515. Epub 2015 May 29. Int J Cancer. 2015. PMID: 25765738 Free PMC article.
-
Local TLR4 stimulation augments in situ vaccination induced via local radiation and anti-CTLA-4 checkpoint blockade through induction of CD8 T-cell independent Th1 polarization.J Immunother Cancer. 2022 Oct;10(10):e005103. doi: 10.1136/jitc-2022-005103. J Immunother Cancer. 2022. PMID: 36192087 Free PMC article.
-
ILC2-driven innate immune checkpoint mechanism antagonizes NK cell antimetastatic function in the lung.Nat Immunol. 2020 Sep;21(9):998-1009. doi: 10.1038/s41590-020-0745-y. Epub 2020 Aug 3. Nat Immunol. 2020. PMID: 32747815 Free PMC article.
-
CAR-T cell therapy: a game-changer in cancer treatment and beyond.Clin Transl Oncol. 2024 Jun;26(6):1300-1318. doi: 10.1007/s12094-023-03368-2. Epub 2024 Jan 20. Clin Transl Oncol. 2024. PMID: 38244129 Review.
References
-
- Acuto O, Michel F. CD28-mediated costimulation: A quantitative support for TCR signalling. Nat Rev Immunol. 2003;3:939–951. - PubMed
-
- Aramaki O, Shirasugi N, Takayama T, Shimazu M, Kitajima M, Ikeda Y, Azuma M, Okumura K, Yagita H, Niimi M. Programmed death-1-programmed death-L1 interaction is essential for induction of regulatory cells by intratracheal delivery of alloantigen. Transplantation. 2004;77:6–12. - PubMed
-
- Atkins MB, Lotze MT, Dutcher JP, Fisher RI, Weiss G, Margolin K, Abrams J, Sznol M, Parkinson D, Hawkins M, Paradise C, Kunkel L, Rosenberg SA. High-dose recombinant interleukin 2 therapy for patients with metastatic melanoma: Analysis of 270 patients treated between 1985 and 1993. J Clin Oncol. 1999;17:2105–2116. - PubMed
-
- Attia P, Phan GQ, Maker AV, Robinson MR, Quezado MM, Yang JC, Sherry RM, Topalian SL, Kammula US, Royal RE, Restifo NP, Haworth LR, et al. Autoimmunity correlates with tumor regression in patients with metastatic melanoma treated with anti-cytotoxic T-lymphocyte antigen-4. J Clin Oncol. 2005;23:6043–6053. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
