

Multiple organ infection and the pathogenesis of SARS
- PMID: 16043521
- PMCID: PMC2213088
- DOI: 10.1084/jem.20050828
Multiple organ infection and the pathogenesis of SARS
Abstract
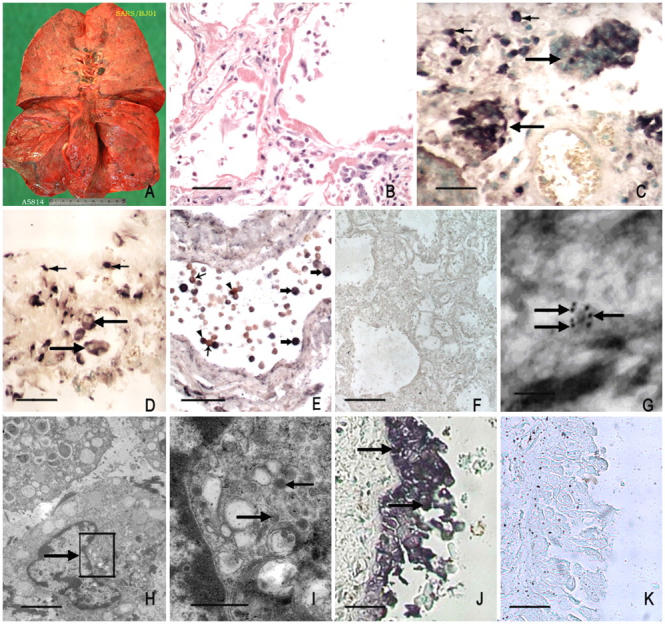
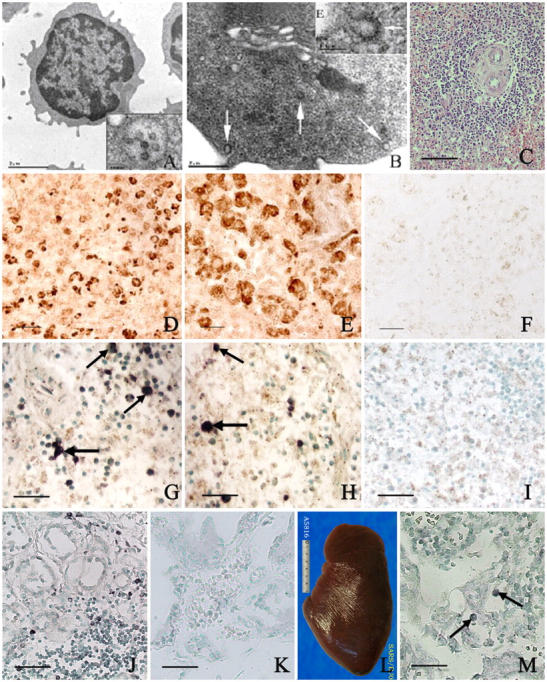
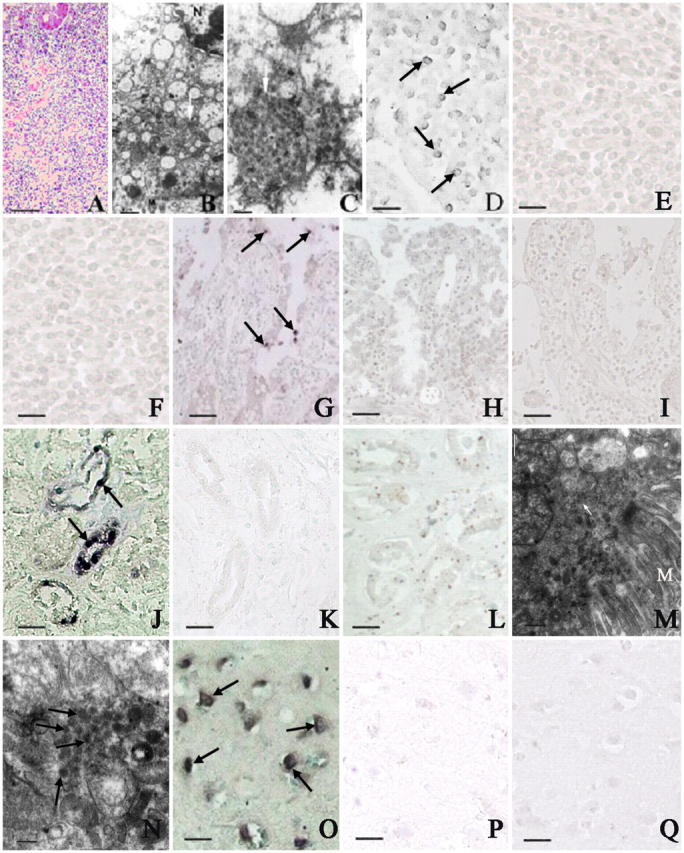
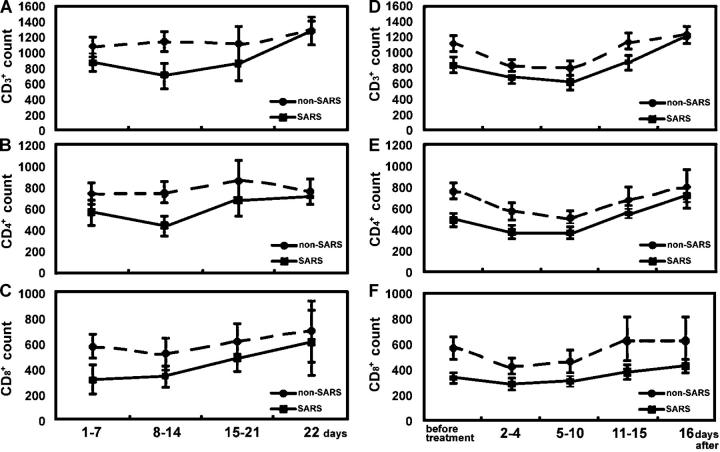
After >8,000 infections and >700 deaths worldwide, the pathogenesis of the new infectious disease, severe acute respiratory syndrome (SARS), remains poorly understood. We investigated 18 autopsies of patients who had suspected SARS; 8 cases were confirmed as SARS. We evaluated white blood cells from 22 confirmed SARS patients at various stages of the disease. T lymphocyte counts in 65 confirmed and 35 misdiagnosed SARS cases also were analyzed retrospectively. SARS viral particles and genomic sequence were detected in a large number of circulating lymphocytes, monocytes, and lymphoid tissues, as well as in the epithelial cells of the respiratory tract, the mucosa of the intestine, the epithelium of the renal distal tubules, the neurons of the brain, and macrophages in different organs. SARS virus seemed to be capable of infecting multiple cell types in several organs; immune cells and pulmonary epithelium were identified as the main sites of injury. A comprehensive theory of pathogenesis is proposed for SARS with immune and lung damage as key features.
Figures
Similar articles
-
[Clinical pathology and pathogenesis of severe acute respiratory syndrome].Zhonghua Shi Yan He Lin Chuang Bing Du Xue Za Zhi. 2003 Sep;17(3):217-21. Zhonghua Shi Yan He Lin Chuang Bing Du Xue Za Zhi. 2003. PMID: 15340561 Chinese.
-
[Lung pathology and pathogenesis of severe acute respiratory syndrome: a report of six full autopsies].Zhonghua Bing Li Xue Za Zhi. 2005 Oct;34(10):656-60. Zhonghua Bing Li Xue Za Zhi. 2005. PMID: 16536279 Chinese.
-
In situ detection of SARS-CoV-2 in lungs and airways of patients with COVID-19.Mod Pathol. 2020 Nov;33(11):2104-2114. doi: 10.1038/s41379-020-0595-z. Epub 2020 Jun 19. Mod Pathol. 2020. PMID: 32561849 Free PMC article.
-
Pathogenetic mechanisms of severe acute respiratory syndrome.Virus Res. 2008 Apr;133(1):4-12. doi: 10.1016/j.virusres.2007.01.022. Epub 2007 Sep 7. Virus Res. 2008. PMID: 17825937 Free PMC article. Review.
-
SARS-CoV replication and pathogenesis in an in vitro model of the human conducting airway epithelium.Virus Res. 2008 Apr;133(1):33-44. doi: 10.1016/j.virusres.2007.03.013. Epub 2007 Apr 23. Virus Res. 2008. PMID: 17451829 Free PMC article. Review.
Cited by
-
T Regulatory Cell Subsets Do Not Restore for One Year After Acute COVID-19.Int J Mol Sci. 2024 Nov 1;25(21):11759. doi: 10.3390/ijms252111759. Int J Mol Sci. 2024. PMID: 39519310 Free PMC article.
-
Serum proteomics for the identification of biomarkers to flag predilection of COVID19 patients to various organ morbidities.Clin Proteomics. 2024 Nov 1;21(1):61. doi: 10.1186/s12014-024-09512-6. Clin Proteomics. 2024. PMID: 39487396 Free PMC article.
-
The role of Helicobacter pylori in augmenting the severity of SARS-CoV-2 related gastrointestinal symptoms: An insight from molecular mechanism of co-infection.Heliyon. 2024 Sep 17;10(18):e37585. doi: 10.1016/j.heliyon.2024.e37585. eCollection 2024 Sep 30. Heliyon. 2024. PMID: 39364240 Free PMC article.
-
Cytokine Storm-Induced Thyroid Dysfunction in COVID-19: Insights into Pathogenesis and Therapeutic Approaches.Drug Des Devel Ther. 2024 Sep 20;18:4215-4240. doi: 10.2147/DDDT.S475005. eCollection 2024. Drug Des Devel Ther. 2024. PMID: 39319193 Free PMC article. Review.
-
Addressing Long COVID Sequelae and Neurocovid: Neuropsychological Scenarios and Neuroimaging Findings.Adv Exp Med Biol. 2024;1457:143-164. doi: 10.1007/978-3-031-61939-7_8. Adv Exp Med Biol. 2024. PMID: 39283425 Review.
References
-
- Peiris, J.S., K.Y. Yuen, A.D. Osterhaus, and K. Stohr. 2003. The severe acute respiratory syndrome. N. Engl. J. Med. 349:2431–2441. - PubMed
-
- World Health Organization. Communicable Disease Surveillance & Response (CSR). Severe Acute Respiratory Syndrome (SARS). Available at: http://www.who.int/csr/sars/en (accessed July 11, 2005).
-
- To, K.F., J.H. Tong, P.K. Chan, F.W. Au, S.S. Chim, K.C. Chan, J.L. Cheung, E.Y. Liu, G.M. Tse, A.W. Lo, et al. 2004. Tissue and cellular tropism of the coronavirus associated with severe acute respiratory syndrome: an in-situ hybridization study of fatal cases. J. Pathol. 202:157–163. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
