

Comparison of CT and three MR sequences for detecting and categorizing early (48 hours) hemorrhagic transformation in hyperacute ischemic stroke
- PMID: 15205127
- PMCID: PMC7975678
Comparison of CT and three MR sequences for detecting and categorizing early (48 hours) hemorrhagic transformation in hyperacute ischemic stroke
Abstract
Background and purpose: Our goal was to compare the sensitivity of CT and three MR sequences in detecting and categorizing early (48 hours) hemorrhagic transformation (HT) in hyperacute ischemic stroke.
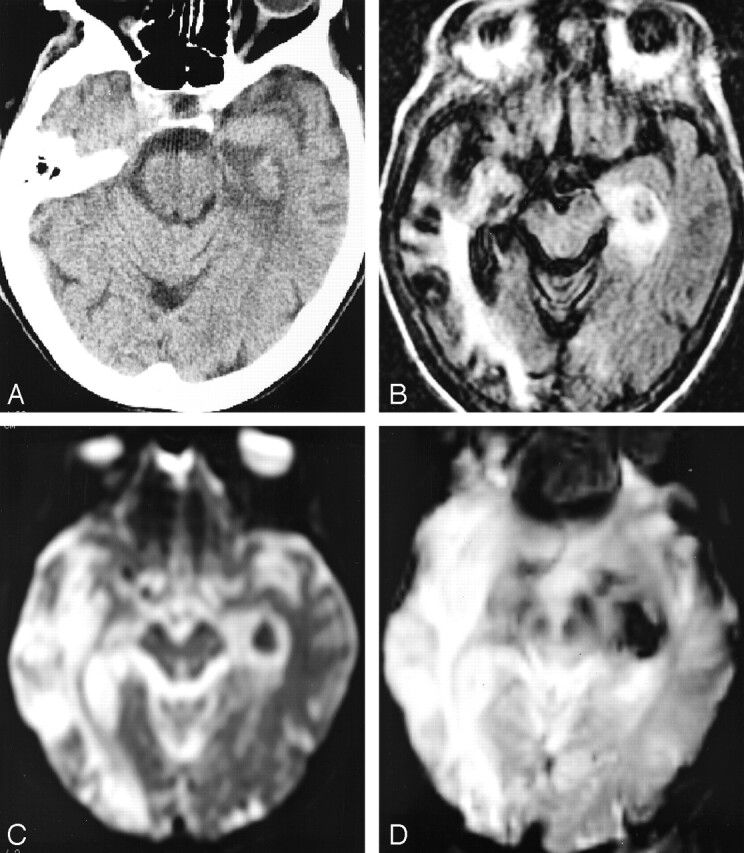
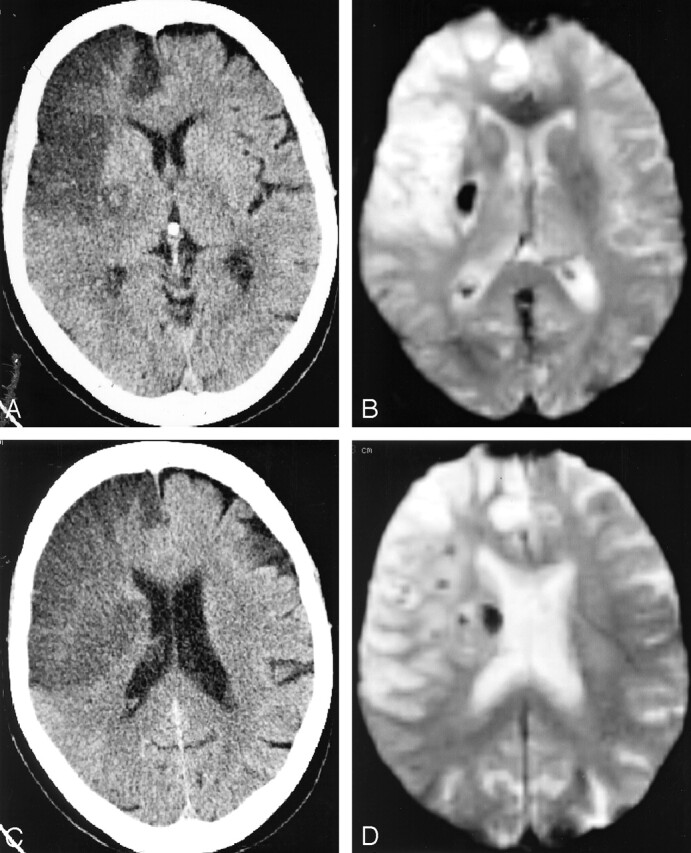
Methods: Twenty-five consecutive patients with hyperacute ischemic stroke (<6 hours) without MR signs of cerebral bleeding at admission were included. Twenty-one underwent thrombolytic therapy. A standardized follow-up protocol, performed 48 hours after admission, combined brain CT scan and MR examination (1.5 T) including fast spin-echo-fluid-attenuated inversion recovery (FSE-FLAIR), echo-planar spin-echo (EPI-SE) T2-weighted, and EPI-gradient-recalled echo (GRE) T2*-weighted sequences. Both CT scans and MR images were obtained within as short a time span as possible between techniques (mean delay, 64 minutes). CT scans and MR images were independently rated as negative or positive for bleeding and categorized for bleeding severity (five classes) by two blinded observers. Prevalence of positive cases, intra- and interobserver agreement, and shifts in bleeding categorization between respective modalities and sequences were assessed.
Results: Twelve patients (48%) were rated positive for HT on the basis of findings of at least one technique or sequence. From this subset of bleeding patients, seven (58%) had positive CT findings, nine (75%) had positive FSE-FLAIR and EPI-SE T2-weighted findings, and 12 (100%) had positive EPI-GRE T2*-weighted findings. CT had lower intra- and interobserver agreement for positivity than did MR imaging. Among the seven patients with positive CT and MR findings, only two had convergent ratings for bleeding category based on findings of two modalities. The five remaining had upward grading from CT to MR, which varied according to pulse sequence.
Conclusion: MR imaging depicted more hemorrhages and had higher intra- and interobserver agreement than did CT. The EPI-GRE T2*-weighted sequence demonstrated highest sensitivity. Equivocal upward shifts in bleeding categorization were observed from CT to MR imaging and between MR images.
Figures

Similar articles
-
Hyperacute intraventricular hemorrhage: detection and characterization, a comparison between 5 MRI sequences.J Neuroradiol. 2007 Mar;34(1):42-8. doi: 10.1016/j.neurad.2007.01.001. J Neuroradiol. 2007. PMID: 17316797
-
MRI of acute post-ischemic cerebral hemorrhage in stroke patients: diagnosis with T2*-weighted gradient-echo sequences.Neuroradiology. 2001 Oct;43(10):809-15. doi: 10.1007/s002340100601. Neuroradiology. 2001. PMID: 11688694
-
Detection of intracranial hemorrhage: comparison between gradient-echo images and b(0) images obtained from diffusion-weighted echo-planar sequences.AJNR Am J Neuroradiol. 2001 Aug;22(7):1275-81. AJNR Am J Neuroradiol. 2001. PMID: 11498414 Free PMC article.
-
Advanced neuroimaging to guide acute stroke therapy.Curr Cardiol Rep. 2012 Dec;14(6):741-53. doi: 10.1007/s11886-012-0315-5. Curr Cardiol Rep. 2012. PMID: 23001815 Review.
-
Non-invasive imaging of intracranial pediatric vascular lesions.Childs Nerv Syst. 2010 Oct;26(10):1275-95. doi: 10.1007/s00381-010-1203-1. Epub 2010 Jul 2. Childs Nerv Syst. 2010. PMID: 20596870 Review.
Cited by
-
Determinants and Clinical Relevance of Iodine Contrast Extravasation after Endovascular Thrombectomy: A Dual-Energy CT Study.AJNR Am J Neuroradiol. 2023 Dec 29;45(1):30-36. doi: 10.3174/ajnr.A8081. AJNR Am J Neuroradiol. 2023. PMID: 38323978 Free PMC article.
-
Hemorrhagic Transformation After Ischemic Stroke: Mechanisms and Management.Front Neurol. 2021 Nov 30;12:703258. doi: 10.3389/fneur.2021.703258. eCollection 2021. Front Neurol. 2021. PMID: 34917010 Free PMC article. Review.
-
Reliability of fast magnetic resonance imaging for acute ischemic stroke patients using a 1.5-T scanner.Eur Radiol. 2019 May;29(5):2641-2650. doi: 10.1007/s00330-018-5812-5. Epub 2018 Nov 12. Eur Radiol. 2019. PMID: 30421013
-
Focal Low and Global High Permeability Predict the Possibility, Risk, and Location of Hemorrhagic Transformation following Intra-Arterial Thrombolysis Therapy in Acute Stroke.AJNR Am J Neuroradiol. 2017 Sep;38(9):1730-1736. doi: 10.3174/ajnr.A5287. Epub 2017 Jul 13. AJNR Am J Neuroradiol. 2017. PMID: 28705822 Free PMC article.
-
Mismatch of Low Perfusion and High Permeability Predicts Hemorrhagic Transformation Region in Acute Ischemic Stroke Patients Treated with Intra-arterial Thrombolysis.Sci Rep. 2016 Jun 15;6:27950. doi: 10.1038/srep27950. Sci Rep. 2016. PMID: 27302077 Free PMC article.
References
-
- The NINDS rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Eng J Med 1995;333:1581–1587 - PubMed
-
- Hacke W, Kaste M, Fieschi C, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke: the European Cooperative Acute Stroke Study (ECASS). JAMA 1995;274:1017–1025 - PubMed
-
- Hacke W, Kaste M, Fieschi C, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Lancet 1998;352:1245–1251 - PubMed
-
- Liu M, Counsell C, Zhao XL, Wardlaw J. Fibrinogen depleting agents for acute ischaemic stroke. In: Cochrane Library Issue 2, Chichester UK: John Wiley and Sons, Ltd.,2004
-
- Fisher CM, Adams RD. Observation on brain embolism with special reference to the mechanism of hemorrhagic infarction. J Neuropathol Exp Neurol 1951;10:92–94 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical