

Tumor microsatellite-instability status as a predictor of benefit from fluorouracil-based adjuvant chemotherapy for colon cancer
- PMID: 12867608
- PMCID: PMC3584639
- DOI: 10.1056/NEJMoa022289
Tumor microsatellite-instability status as a predictor of benefit from fluorouracil-based adjuvant chemotherapy for colon cancer
Abstract
Background: Colon cancers with high-frequency microsatellite instability have clinical and pathological features that distinguish them from microsatellite-stable tumors. We investigated the usefulness of microsatellite-instability status as a predictor of the benefit of adjuvant chemotherapy with fluorouracil in stage II and stage III colon cancer.
Methods: Tumor specimens were collected from patients with colon cancer who were enrolled in randomized trials of fluorouracil-based adjuvant chemotherapy. Microsatellite instability was assessed with the use of mononucleotide and dinucleotide markers.
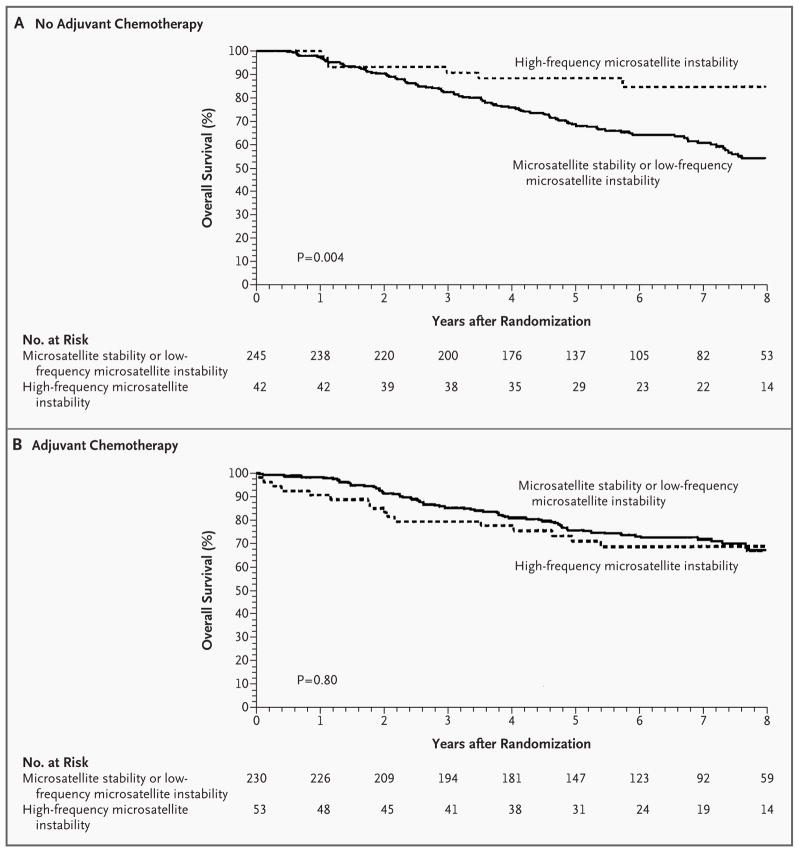
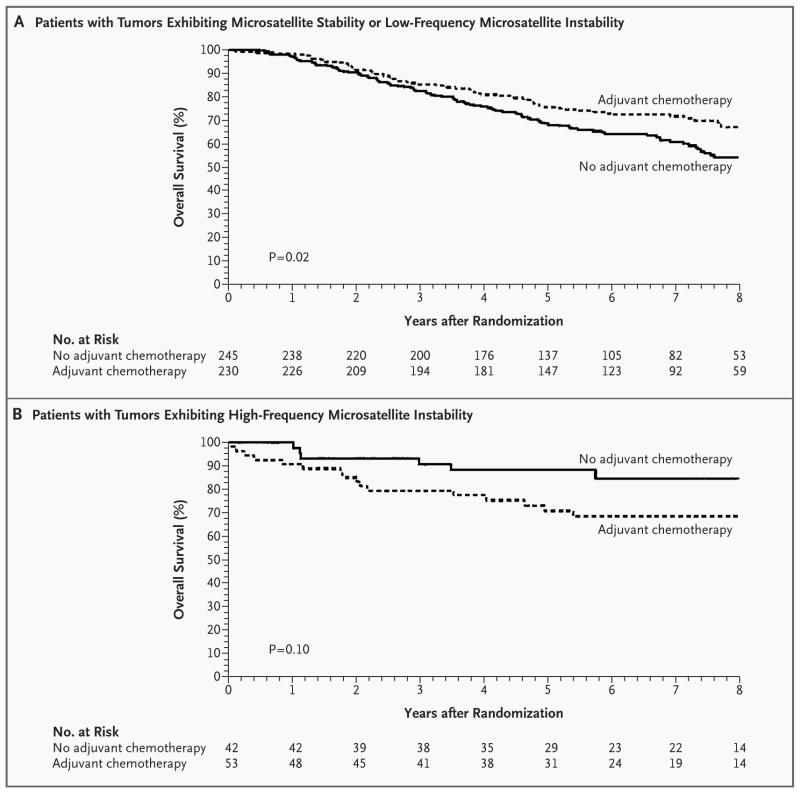
Results: Of 570 tissue specimens, 95 (16.7 percent) exhibited high-frequency microsatellite instability. Among 287 patients who did not receive adjuvant therapy, those with tumors displaying high-frequency microsatellite instability had a better five-year rate of overall survival than patients with tumors exhibiting microsatellite stability or low-frequency instability (hazard ratio for death, 0.31 [95 percent confidence interval, 0.14 to 0.72]; P=0.004). Among patients who received adjuvant chemotherapy, high-frequency microsatellite instability was not correlated with increased overall survival (hazard ratio for death, 1.07 [95 percent confidence interval, 0.62 to 1.86]; P=0.80). The benefit of treatment differed significantly according to the microsatellite-instability status (P=0.01). Adjuvant chemotherapy improved overall survival among patients with microsatellite-stable tumors or tumors exhibiting low-frequency microsatellite instability, according to a multivariate analysis adjusted for stage and grade (hazard ratio for death, 0.72 [95 percent confidence interval, 0.53 to 0.99]; P=0.04). By contrast, there was no benefit of adjuvant chemotherapy in the group with high-frequency microsatellite instability.
Conclusions: Fluorouracil-based adjuvant chemotherapy benefited patients with stage II or stage III colon cancer with microsatellite-stable tumors or tumors exhibiting low-frequency microsatellite instability but not those with tumors exhibiting high-frequency microsatellite instability.
Copyright 2003 Massachusetts Medical Society
Figures
Comment in
-
Microsatellite instability.N Engl J Med. 2003 Jul 17;349(3):209-10. doi: 10.1056/NEJMp038099. N Engl J Med. 2003. PMID: 12867603 No abstract available.
-
Microsatellite instability in colon cancer.N Engl J Med. 2003 Oct 30;349(18):1774-6; author reply 1774-6. doi: 10.1056/NEJM200310303491818. N Engl J Med. 2003. PMID: 14585950 No abstract available.
-
Microsatellite instability in colon cancer.N Engl J Med. 2003 Oct 30;349(18):1774-6; author reply 1774-6. N Engl J Med. 2003. PMID: 14593997 No abstract available.
-
Microsatellite instability in colon cancer.N Engl J Med. 2003 Oct 30;349(18):1774-6; author reply 1774-6. N Engl J Med. 2003. PMID: 14593998 No abstract available.
Similar articles
-
Carcinoma microsatellite instability status as a predictor of benefit from fluorouracil-based adjuvant chemotherapy for stage II rectal cancer.Asian Pac J Cancer Prev. 2015;16(4):1545-51. doi: 10.7314/apjcp.2015.16.4.1545. Asian Pac J Cancer Prev. 2015. PMID: 25743829 Clinical Trial.
-
Microsatellite instability is a predictive marker for survival benefit from adjuvant chemotherapy in a population-based series of stage III colorectal carcinoma.Clin Colorectal Cancer. 2001 Aug;1(2):104-9. doi: 10.3816/CCC.2001.n.010. Clin Colorectal Cancer. 2001. PMID: 12445368
-
Use of 5-fluorouracil and survival in patients with microsatellite-unstable colorectal cancer.Gastroenterology. 2004 Feb;126(2):394-401. doi: 10.1053/j.gastro.2003.12.023. Gastroenterology. 2004. PMID: 14762775
-
Lack of benefit of 5-fluorouracil-based adjuvant chemotherapy in colorectal cancer with microsatellite instability.Clin Colorectal Cancer. 2002 Nov;2(3):146-8. doi: 10.1016/S1533-0028(11)70320-6. Clin Colorectal Cancer. 2002. PMID: 12482330 Review. No abstract available.
-
Biologic behavior of microsatellite-unstable colorectal cancer and treatment with 5-fluorouracil.Isr Med Assoc J. 2005 Aug;7(8):520-4. Isr Med Assoc J. 2005. PMID: 16106779 Review.
Cited by
-
Villin expression is frequently lost in poorly differentiated colon cancer.Am J Pathol. 2012 Apr;180(4):1509-21. doi: 10.1016/j.ajpath.2012.01.006. Epub 2012 Feb 18. Am J Pathol. 2012. PMID: 22349300 Free PMC article.
-
A network-based gene expression signature informs prognosis and treatment for colorectal cancer patients.PLoS One. 2012;7(7):e41292. doi: 10.1371/journal.pone.0041292. Epub 2012 Jul 23. PLoS One. 2012. PMID: 22844451 Free PMC article.
-
Aberrant protein expression and frequent allelic loss of MSH3 in colorectal cancer with low-level microsatellite instability.Int J Colorectal Dis. 2012 Jul;27(7):911-9. doi: 10.1007/s00384-011-1408-0. Epub 2012 Jan 10. Int J Colorectal Dis. 2012. PMID: 22249440
-
WNT5a in Colorectal Cancer: Research Progress and Challenges.Cancer Manag Res. 2021 Mar 16;13:2483-2498. doi: 10.2147/CMAR.S289819. eCollection 2021. Cancer Manag Res. 2021. PMID: 33758546 Free PMC article. Review.
-
Microsatellite instable vs stable colon carcinomas: analysis of tumour heterogeneity, inflammation and angiogenesis.Br J Cancer. 2015 Jul 28;113(3):500-9. doi: 10.1038/bjc.2015.213. Epub 2015 Jun 11. Br J Cancer. 2015. PMID: 26068398 Free PMC article.
References
-
- Miller BA, Kolonel LN, Bernstein L, et al. Racial/ethnic patterns of cancer in the United States 1988–1992. Bethesda, Md: National Cancer Institute; 1996. (NIH publication no. 96-4104.)
-
- Makela JT, Laitinen ST, Kairaluoma MI. Five-year follow-up after radical surgery for colorectal cancer: results of a prospective randomized trial. Arch Surg. 1995;130:1062–7. - PubMed
-
- Obrand DI, Gordon PH. Incidence and patterns of recurrence following curative resection for colorectal carcinoma. Dis Colon Rectum. 1997;40:15–24. - PubMed
-
- International Multicentre Pooled Analysis of Colon Cancer Trials (IMPACT) Investigators. Efficacy of adjuvant fluorouracil and folinic acid in colon cancer. Lancet. 1995;345:939–44. - PubMed
-
- Moertel CG, Fleming TR, Macdonald JS, et al. Levamisole and fluorouracil for adjuvant therapy of resected colon carcinoma. N Engl J Med. 1990;322:352–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical