

Variation in death rate after abdominal aortic aneurysmectomy in the United States: impact of hospital volume, gender, and age
- PMID: 11923615
- PMCID: PMC1422474
- DOI: 10.1097/00000658-200204000-00017
Variation in death rate after abdominal aortic aneurysmectomy in the United States: impact of hospital volume, gender, and age
Abstract
Objective: To determine whether high-volume hospitals (HVHs) have lower in-hospital death rates after abdominal aortic aneurysm (AAA) repair compared with low-volume hospitals (LVHs).
Summary background data: Select statewide studies have shown that HVHs have superior outcomes compared with LVHs for AAA repair, but they may not be representative of the true volume-outcome relationship for the entire United States.
Methods: Patients undergoing repair of intact or ruptured AAAs in the Nationwide Inpatient Sample (NIS) for 1996 and 1997 were included (n = 13,887) for study. The NIS represents a 20% stratified random sample representative of all U.S. hospitals. Unadjusted and case mix-adjusted analyses were performed.
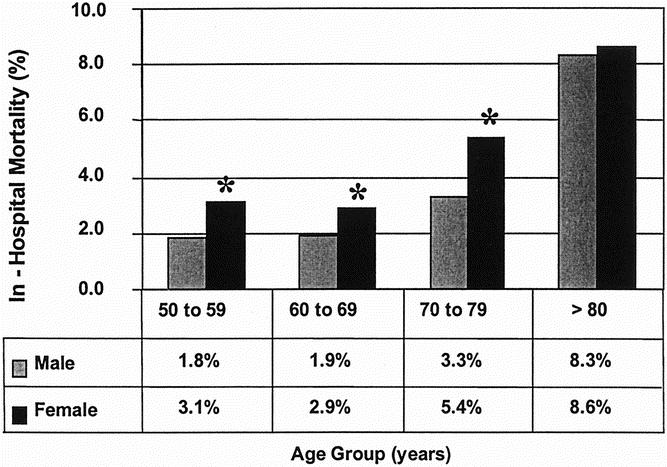
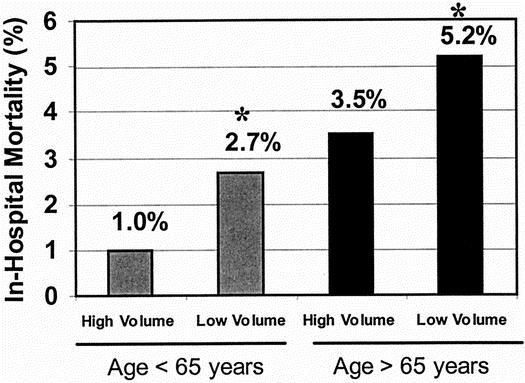
Results: The overall death rate was 3.8% for intact AAA repair and 47% for ruptured AAA repair. For repair of intact AAAs, HVHs had a lower death rate than LVHs. The death rate after repair of ruptured AAA was also slightly lower at HVHs. In a multivariate analysis adjusting for case mix, having surgery at an LVH was associated with a 56% increased risk of in-hospital death. Other independent risk factors for in-hospital death included female gender, age older than 65 years, aneurysm rupture, urgent or emergent admission, and comorbid disease.
Conclusions: This study from a representative national database documents that HVHs have a significantly lower death rate than LVHs for repair of both intact and ruptured AAA. These data support the regionalization of patients to HVHs for AAA repair.
Figures
Comment in
-
Aortic aneurysms: an update.Curr Surg. 2003 May-Jun;60(3):246-51. doi: 10.1016/s0149-7944(02)00790-0. Curr Surg. 2003. PMID: 15212058 No abstract available.
Similar articles
-
The effect of hospital factors on mortality rates after abdominal aortic aneurysm repair.J Vasc Surg. 2014 Dec;60(6):1446-51. doi: 10.1016/j.jvs.2014.08.111. Epub 2014 Oct 14. J Vasc Surg. 2014. PMID: 25441675
-
The Agency for Healthcare Research and Quality Inpatient Quality Indicator #11 overall mortality rate does not accurately assess mortality risk after abdominal aortic aneurysm repair.J Vasc Surg. 2015 Jan;61(1):44-9. doi: 10.1016/j.jvs.2014.06.106. Epub 2014 Jul 24. J Vasc Surg. 2015. PMID: 25065583
-
Abdominal aortic aneurysm repair in Veterans Affairs medical centers.J Vasc Surg. 1996 Feb;23(2):191-200. doi: 10.1016/s0741-5214(96)70263-x. J Vasc Surg. 1996. PMID: 8637096
-
Meta-analysis and systematic review of the relationship between volume and outcome in abdominal aortic aneurysm surgery.Br J Surg. 2007 Apr;94(4):395-403. doi: 10.1002/bjs.5710. Br J Surg. 2007. PMID: 17380547 Review.
-
Is endovascular repair of ruptured abdominal aortic aneurysms associated with improved in-hospital mortality compared with surgical repair?Interact Cardiovasc Thorac Surg. 2015 Jan;20(1):135-9. doi: 10.1093/icvts/ivu329. Epub 2014 Oct 3. Interact Cardiovasc Thorac Surg. 2015. PMID: 25281705 Review.
Cited by
-
Decreased collagen and increased matrix metalloproteinase-13 in experimental abdominal aortic aneurysms in males compared with females.Surgery. 2010 Feb;147(2):258-67. doi: 10.1016/j.surg.2009.06.047. Epub 2009 Sep 20. Surgery. 2010. PMID: 19767051 Free PMC article.
-
A study to characterize the mechanical properties and material constitution of adult descending thoracic aorta based on uniaxial tensile test and digital image correlation.Front Bioeng Biotechnol. 2023 Jun 14;11:1178199. doi: 10.3389/fbioe.2023.1178199. eCollection 2023. Front Bioeng Biotechnol. 2023. PMID: 37388776 Free PMC article.
-
A national and single institutional experience in the contemporary treatment of acute lower extremity ischemia.Ann Surg. 2003 Sep;238(3):382-9; discussion 389-90. doi: 10.1097/01.sla.0000086663.49670.d1. Ann Surg. 2003. PMID: 14501504 Free PMC article.
-
The Challenge of Endoleaks in Endovascular Aneurysm Repair (EVAR): A Review of Their Types and Management.Cureus. 2023 May 31;15(5):e39775. doi: 10.7759/cureus.39775. eCollection 2023 May. Cureus. 2023. PMID: 37398777 Free PMC article. Review.
-
Population-based outcomes following endovascular and open repair of ruptured abdominal aortic aneurysms.J Endovasc Ther. 2009 Oct;16(5):554-64. doi: 10.1583/09-2743.1. J Endovasc Ther. 2009. PMID: 19842719 Free PMC article.
References
-
- Ernst CB. Abdominal aortic aneurysm. N Engl J Med 1993; 328: 1167–1172. - PubMed
-
- Huber TS, Wang JG, Derrow AE, et al. Experience in the United States with intact abdominal aortic aneurysm repair. J Vasc Surg 2001; 33: 304–311. - PubMed
-
- Luft HS, Bunker JP, Enthoven AC. Should operations be regionalized? The empirical relationship between surgical volume and mortality. N Engl J Med 1979; 301: 1364–1369. - PubMed
-
- Dudley RA, Johansen KL, Brand R, et al. Selective referral to high-volume hospitals: estimating potentially avoidable deaths. JAMA 2000; 283: 1159–1166. - PubMed
-
- Wennberg DE, Lucas FL, Birkmeyer JD, et al. Variation in carotid endarterectomy mortality in the Medicare population. JAMA 1998; 279: 1278–1281. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
