

The cutaneous uptake of atmospheric oxygen contributes significantly to the oxygen supply of human dermis and epidermis
- PMID: 11826181
- PMCID: PMC2290093
- DOI: 10.1113/jphysiol.2001.013067
The cutaneous uptake of atmospheric oxygen contributes significantly to the oxygen supply of human dermis and epidermis
Abstract
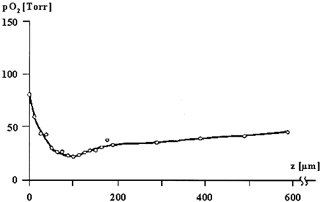
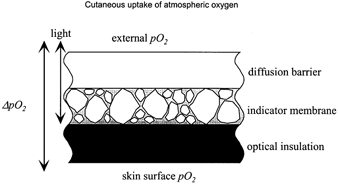
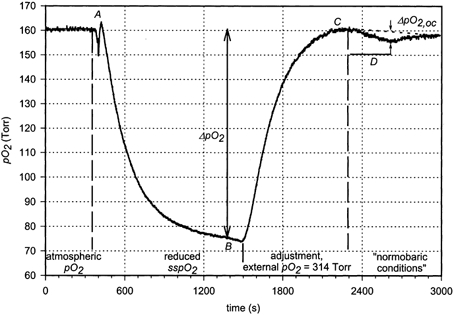
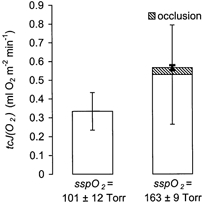
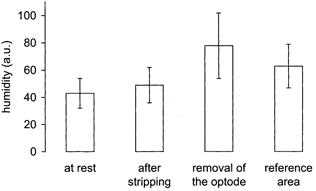
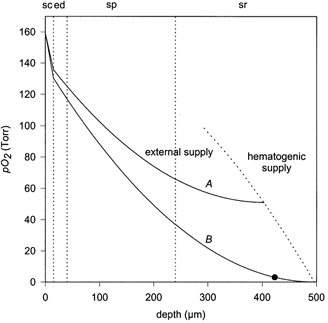
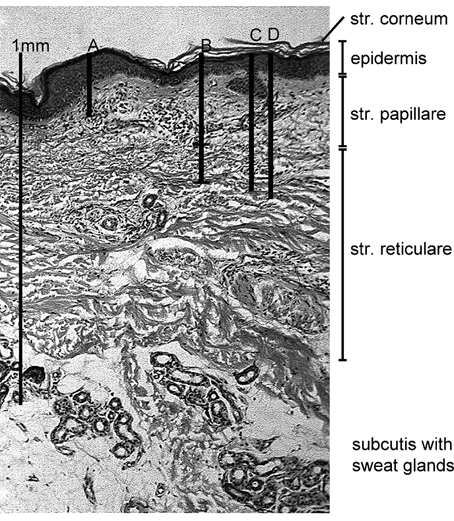
It has been known since 1851 that atmospheric oxygen is taken up by the human epidermis. The contribution to total respiration is negligible. Until now the significance for the local oxygen supply of the skin has remained unknown. With a newly developed sensor, the oxygen fluxoptode, it has become possible to make local measurements of the transcutaneous oxygen flux (tcJ(O2)). In this study the sensor was calibrated so that absolute values of tcJ(O2) could be reported. At rest, tcJ(O2) was determined on normal, humidified skin on the volar forearm of 20 volunteers of different age groups. In order to evaluate the contribution of the blood flow to the oxygen supply of the skin, tcJ(O2) was recorded at the end of a 5 min suprasystolic occlusion of the forearm. At normal skin surface partial oxygen pressure (163 +/- 9 Torr), tcJ(O2) was 0.53 +/- 0.27 ml O2 min(-1) x m(-2). A 5 min interruption of blood flow resulted in an increase of 9.5 +/- 6.3 % in tcJ(O2). The value of tcJ(O2) was unaffected by the age of the subject. Published data on the oxygen diffusion properties of skin and simulations of intracutaneous profiles of oxygen partial pressure indicated that under these conditions, the upper skin layers to a depth of of 0.25-0.40 mm are almost exclusively supplied by external oxygen, whereas the oxygen transport of the blood has a minor influence. As a consequence, a malfunction in capillary oxygen transport cannot be the initiator of the development of superficial skin defects such as those observed in chronic venous incompetence and peripheral arterial occlusive disease.
Figures
Similar articles
-
The transepidermal oxygen flux from the environment is in balance with the capillary oxygen supply.J Invest Dermatol. 2000 Mar;114(3):533-40. doi: 10.1046/j.1523-1747.2000.00911.x. J Invest Dermatol. 2000. PMID: 10692114
-
A new measuring device for non-invasive determination of oxygen partial pressure and oxygen conductance of the skin and other tissues.Adv Exp Med Biol. 1999;471:705-14. doi: 10.1007/978-1-4615-4717-4_81. Adv Exp Med Biol. 1999. PMID: 10659205
-
Oxygen tension and consumption measured by a tc-PO2 electrode on heated skin before and after epidermal stripping.Acta Anaesthesiol Scand. 1987 Jul;31(5):362-9. doi: 10.1111/j.1399-6576.1987.tb02585.x. Acta Anaesthesiol Scand. 1987. PMID: 3630579
-
Skin oxygen tension, skin oxygen consumption, and skin blood flow measured by a tc-pO2 electrode.Acta Physiol Scand Suppl. 1991;603:53-7. Acta Physiol Scand Suppl. 1991. PMID: 1789131 Review.
-
Blood flow rate, temperature, oxygen tension and consumption in the skin of adults measured by a heated microcathode oxygen electrode.Dan Med Bull. 1988 Aug;35(4):322-34. Dan Med Bull. 1988. PMID: 3048920 Review.
Cited by
-
Functional respiratory morphology in the newborn quokka wallaby (Setonix brachyurus).J Anat. 2007 Jul;211(1):26-36. doi: 10.1111/j.1469-7580.2007.00744.x. Epub 2007 Jun 6. J Anat. 2007. PMID: 17553103 Free PMC article.
-
Enhancing the longevity of microparticle-based glucose sensors towards 1 month continuous operation.Biosens Bioelectron. 2010 Jan 15;25(5):1075-81. doi: 10.1016/j.bios.2009.09.026. Epub 2009 Oct 12. Biosens Bioelectron. 2010. PMID: 19926464 Free PMC article.
-
The Mitochondrial Respiratory Chain Is Required for Organismal Adaptation to Hypoxia.Cell Rep. 2016 Apr 19;15(3):451-459. doi: 10.1016/j.celrep.2016.03.044. Epub 2016 Apr 7. Cell Rep. 2016. PMID: 27068470 Free PMC article.
-
How might we achieve oxygen balance in wounds?Int Wound J. 2007 Sep;4 Suppl 3(Suppl 3):18-24. doi: 10.1111/j.1742-481X.2007.00384.x. Int Wound J. 2007. PMID: 17894664 Free PMC article.
-
Computational models of melanoma.Theor Biol Med Model. 2020 May 14;17(1):8. doi: 10.1186/s12976-020-00126-7. Theor Biol Med Model. 2020. PMID: 32410672 Free PMC article. Review.
References
-
- Aiba S, Ohashi M, Huang SY. Rapid determination of oxygen permeability of polymer membranes. Industrial and Engineering Chemistry Fundamentals. 1968;7:497–502.
-
- Balin AK, Lin AN. Skin changes as a biological marker for measuring the rate of human aging. In: Balin AK, Kligman AM, editors. Aging and the Skin. New York: Raven; 1989. pp. 43–75.
-
- Baumgärtl H, Ehrly AM, Saeger-Lorenz K, Lübbers DW. Initial results of intracutaneous measurements of PO2 profiles. In: Ehrly AM, Hauss J, Huch R, editors. Clinical Oxygen Pressure Measurement. Berlin: Springer; 1987. pp. 121–128.
-
- Bongard O, Bounameaux H. Clinical investigation of skin microcirculation. Dermatology. 1993;186:6–11. - PubMed
-
- Braverman IM. Ultrastructure and organization of the cutaneous microvasculature in normal and pathologic states. Journal of Investigative Dermatology. 1989;93:2S–9S. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous