

Epstein-Barr virus and gastric carcinoma
- PMID: 11091849
- PMCID: PMC1186978
- DOI: 10.1136/mp.53.5.255
Epstein-Barr virus and gastric carcinoma
Abstract
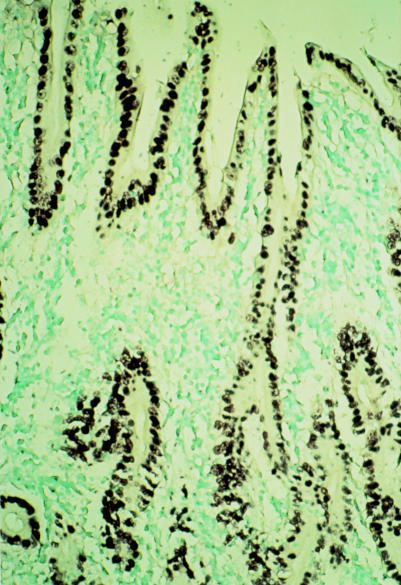
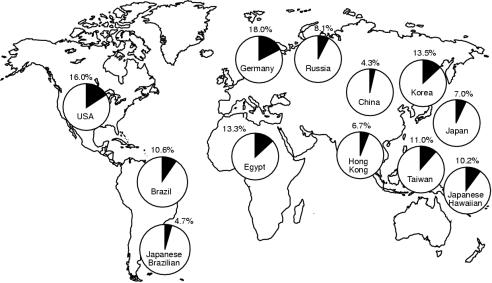
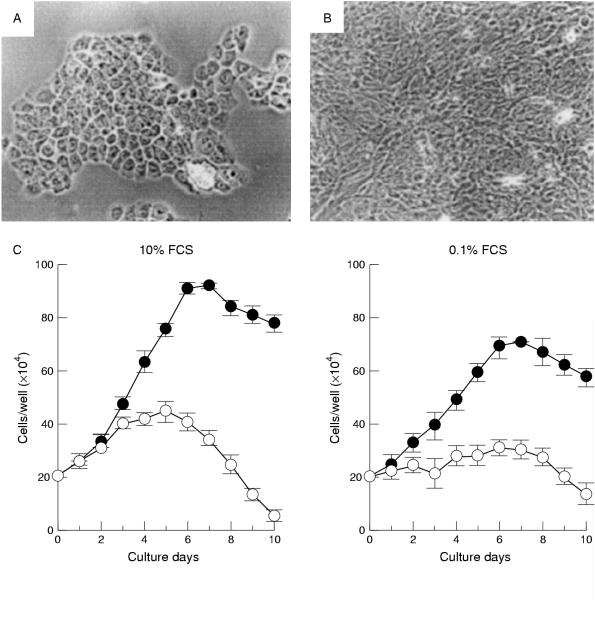
The Epstein-Barr virus (EBV) is detected in the tissue of about 10% of gastric carcinoma cases throughout the world. In each case, 100% of carcinoma cells are infected with EBV. Analysis of EBV in carcinoma biopsies indicates that carcinoma is formed by the proliferation of a single EBV infected cell. These findings suggest that EBV plays an important role in the development of EBV positive gastric carcinomas. The EBV genes expressed are EBV determined nuclear antigen 1 (EBNA1), two small non-polyadenylated RNAs known as EBER1 and EBER2, and the transcripts from the BamHI-A region (BARF0); in addition, some cases also express a small amount of latent membrane protein 2A (LMP2A). Epithelial cells are refractory to EBV infection in vitro. This has hampered the study of the role of EBV in epithelial malignancies. The use of recombinant EBV carrying a selectable marker has enabled this difficulty to be overcome. EBV infected cell clones can be obtained from most carcinoma cell lines examined, and it was found that cell to cell contact was an efficient mode of EBV infection. Furthermore, it was possible to immortalize primary gastric epithelial cells by EBV infection. The cells expressed identical EBV genes to those typically seen in EBV positive gastric carcinoma, and showed accelerated malignant properties, including growth in soft agarose and tumorigenicity in severe combined immunodeficient (SCID) mice. These results suggest that EBV contributes to the maintenance of the malignant phenotype of EBV positive gastric carcinoma.
Figures


Similar articles
-
Detection of transcripts initiated from two viral promoters (Cp and Wp) in Epstein-Barr virus-infected nasopharyngeal carcinoma cells and biopsies.Lab Invest. 1998 Jun;78(6):715-26. Lab Invest. 1998. PMID: 9645762
-
Unique transcription pattern of Epstein-Barr virus (EBV) in EBV-carrying gastric adenocarcinomas: expression of the transforming BARF1 gene.Cancer Res. 2000 May 15;60(10):2745-8. Cancer Res. 2000. PMID: 10825150
-
Characterization of Epstein-Barr virus infection in a human signet ring cell gastric carcinoma cell line, HSC-39.Microbes Infect. 2004 Apr;6(5):429-39. doi: 10.1016/j.micinf.2003.12.017. Microbes Infect. 2004. PMID: 15109957
-
Epstein-Barr virus (EBV) infection and gastric carcinoma: the approach through EBV infected epithelial cell lines.Jpn J Infect Dis. 1999 Jun;52(3):110-2. Jpn J Infect Dis. 1999. PMID: 10507989 Review.
-
[State of art: Epstein Barr virus-associated gastric carcinoma].Nihon Rinsho. 1997 Feb;55(2):357-62. Nihon Rinsho. 1997. PMID: 9046823 Review. Japanese.
Cited by
-
Differential expression of EBV proteins LMP1 and BHFR1 in EBV‑associated gastric and nasopharyngeal cancer tissues.Mol Med Rep. 2016 May;13(5):4151-8. doi: 10.3892/mmr.2016.5087. Epub 2016 Apr 5. Mol Med Rep. 2016. PMID: 27052804 Free PMC article.
-
11. Cancers attributable to infection in the UK in 2010.Br J Cancer. 2011 Dec 6;105 Suppl 2(Suppl 2):S49-56. doi: 10.1038/bjc.2011.484. Br J Cancer. 2011. PMID: 22158321 Free PMC article. No abstract available.
-
Association between Helicobacter pylori, Epstein-Barr virus, human papillomavirus and gastric adenocarcinomas.World J Gastroenterol. 2018 Nov 21;24(43):4928-4938. doi: 10.3748/wjg.v24.i43.4928. World J Gastroenterol. 2018. PMID: 30487702 Free PMC article.
-
Gastric cancer stem cells.J Clin Oncol. 2008 Jun 10;26(17):2876-82. doi: 10.1200/JCO.2007.15.2603. J Clin Oncol. 2008. PMID: 18539967 Free PMC article. Review.
-
Host genetics of Epstein-Barr virus infection, latency and disease.Rev Med Virol. 2015 Mar;25(2):71-84. doi: 10.1002/rmv.1816. Epub 2014 Nov 27. Rev Med Virol. 2015. PMID: 25430668 Free PMC article. Review.
References
-
- Rickinson AB, Kieff E. Epstein-Barr virus. In: Fields BN, Knipe DM, Howley PM, eds. Virology, 3rd ed. Philadelphia: Lippincott-Raven, 1996:2397–446.
-
- Burke AP, Yen TSB, Shekitka KM, et al. Lymphoepithelial carcinoma of the stomach with Epstein-Barr virus demonstrated by polymerase chain reaction. Mod Pathol 1990;3:377–80. - PubMed
-
- Takano Y, Kato Y, Sugano H. Epstein-Barr virus-associated medullary carcinomas with lymphoid infiltration of the stomach. Cancer Res Clin Oncol 1994;120:303–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical