

Impact of highly active anti-retroviral therapy (HAART) on cytokine production and monocyte subsets in HIV-infected patients
- PMID: 10759771
- PMCID: PMC1905601
- DOI: 10.1046/j.1365-2249.2000.01201.x
Impact of highly active anti-retroviral therapy (HAART) on cytokine production and monocyte subsets in HIV-infected patients
Abstract
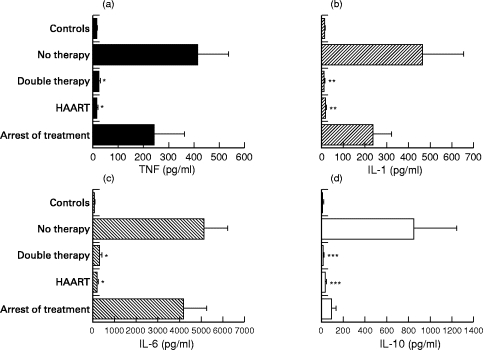
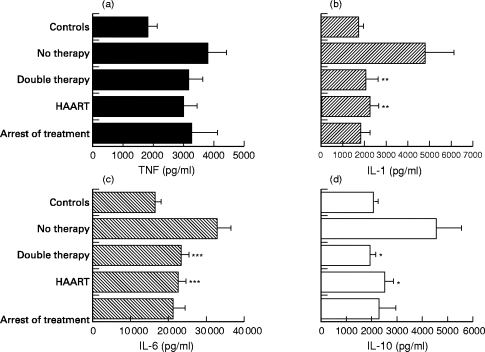
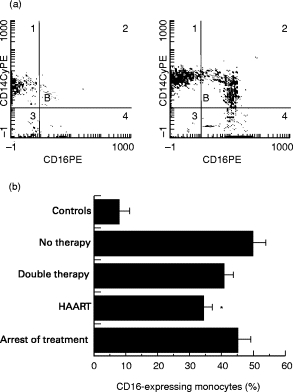
HIV infection is associated with cytokine production by monocytes and expansion of a monocyte subset that expresses high levels of CD16. Our study was designed to investigate the effects of anti-retroviral therapies on these immune parameters. Four groups of HIV+ patients were included in the study. The first group comprised drug-naive patients (n = 20); the second included patients who received two inhibitors of HIV reverse transcriptase (n = 45); the third group received a therapy combining these two inhibitors and one inhibitor of HIV protease (HAART) (n = 35); the fourth consisted of patients who had stopped their treatment (n = 20). The release of inflammatory cytokines (tumour necrosis factor, IL-1beta, IL-6) and immunoregulatory cytokines such as IL-10 by monocytes was determined by ELISA. The monocyte subsets expressing low or high levels of CD16 were studied by flow cytometry. Monocytes from patients naive of treatment released higher amounts of inflammatory cytokines and IL-10 than HIV- individuals. Each anti-retroviral therapy restored a normal pattern of cytokine secretion. Nevertheless, the release of cytokines increased again after the arrest of the treatment. The expansion of the monocyte subset that expresses high levels of CD16 was significantly decreased by HAART but not by the treatment including two inhibitors of reverse transcriptase. These results suggest that only HAART controls monocyte activation in the treatment of HIV infection.
Figures
Similar articles
-
Improvement in neutrophil and monocyte function during highly active antiretroviral treatment of HIV-1-infected patients.AIDS. 1999 May 28;13(8):883-90. doi: 10.1097/00002030-199905280-00003. AIDS. 1999. PMID: 10371168 Clinical Trial.
-
Differences in cellular activation and apoptosis in HIV-infected patients receiving protease inhibitors or nonnucleoside reverse transcriptase inhibitors.AIDS Res Hum Retroviruses. 2002 Dec 10;18(18):1379-88. doi: 10.1089/088922202320935456. AIDS Res Hum Retroviruses. 2002. PMID: 12487809
-
Impact of NNRTI compared to PI-based highly active antiretroviral therapy on CCR5 receptor expression, beta-chemokines and IL-16 secretion in HIV-1 infection.Clin Exp Immunol. 2002 Nov;130(2):286-92. doi: 10.1046/j.1365-2249.2002.01993.x. Clin Exp Immunol. 2002. PMID: 12390317 Free PMC article. Clinical Trial.
-
Salvage therapy for patients failing their current antiretroviral regimen.AIDS Clin Rev. 2000-2001:139-91. AIDS Clin Rev. 2000. PMID: 10999220 Review. No abstract available.
-
[Human immunodeficiency virus and antiretroviral therapy resistance].Enferm Infecc Microbiol Clin. 2000 May;18(5):234-7. Enferm Infecc Microbiol Clin. 2000. PMID: 10974768 Review. Spanish. No abstract available.
Cited by
-
A non-specific biomarker of disease activity in HIV/AIDS patients from resource-limited environments.Afr Health Sci. 2015 Jun;15(2):334-43. doi: 10.4314/ahs.v15i2.5. Afr Health Sci. 2015. PMID: 26124777 Free PMC article.
-
Brain 18F-FDG PET of SIV-infected macaques after treatment interruption or initiation.J Neuroinflammation. 2018 Jul 14;15(1):207. doi: 10.1186/s12974-018-1244-z. J Neuroinflammation. 2018. PMID: 30007411 Free PMC article.
-
The role of monocytes and perivascular macrophages in HIV and SIV neuropathogenesis: information from non-human primate models.Neurotox Res. 2005 Oct;8(1-2):107-15. doi: 10.1007/BF03033823. Neurotox Res. 2005. PMID: 16260389 Review.
-
Effect of Probiotic Supplement on Cytokine Levels in HIV-Infected Individuals: A Preliminary Study.Nutrients. 2015 Sep 28;7(10):8335-47. doi: 10.3390/nu7105396. Nutrients. 2015. PMID: 26426044 Free PMC article.
-
Immune Dysfunction in HIV: A Possible Role for Pro- and Anti-Inflammatory Cytokines in HIV Staging.J Immunol Res. 2017;2017:4128398. doi: 10.1155/2017/4128398. Epub 2017 Nov 2. J Immunol Res. 2017. PMID: 29230423 Free PMC article.
References
-
- Palella FJ, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, Aschman DJ, Holmberg SD. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. N Engl J Med. 1998;338:853–60. - PubMed
-
- Cameron DW, Heath-Chiozzi M, Danner S, et al. Randomised placebo-controlled trial of ritonavir in advanced HIV-1 disease. Lancet. 1998;351:543–9. - PubMed
-
- Collier AC, Coombs RW, Schoenfeld DA, et al. Treatment of human immunodeficiency virus infection with saquinavir, zidovudine, and zalcitabine. N Engl J Med. 1996;334:1011–8. - PubMed
-
- Nielsen SD, Ersboll AK, Mathiesen L, Nielsen JO, Hansen JES. Highly active antiretroviral therapy normalizes the function of progenitor cells in human immunodeficiency virus-infected patients. J Infect Dis. 1998;178:1299–305. - PubMed
-
- Pakker NG, Notermans DW, de Boer RJ, et al. Biphasic kinetics of peripheral blood T cells after triple combination therapy in HIV-1 infection: a composite of redistribution and proliferation. Nature Med. 1998;4:208–14. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
