

VEGF localisation in diabetic retinopathy
- PMID: 9713066
- PMCID: PMC1722605
- DOI: 10.1136/bjo.82.5.561
VEGF localisation in diabetic retinopathy
Abstract
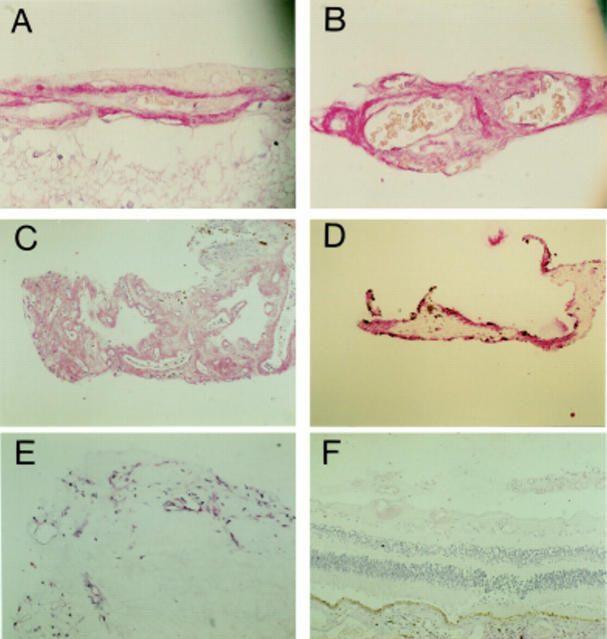
Aim: To determine the staining pattern of vascular endothelial growth factor (VEGF) at different stages of diabetic retinopathy (including post-laser photocoagulation) and to compare staining in excised fibrovascular and fibrocellular (non-diabetic) preretinal membranes.
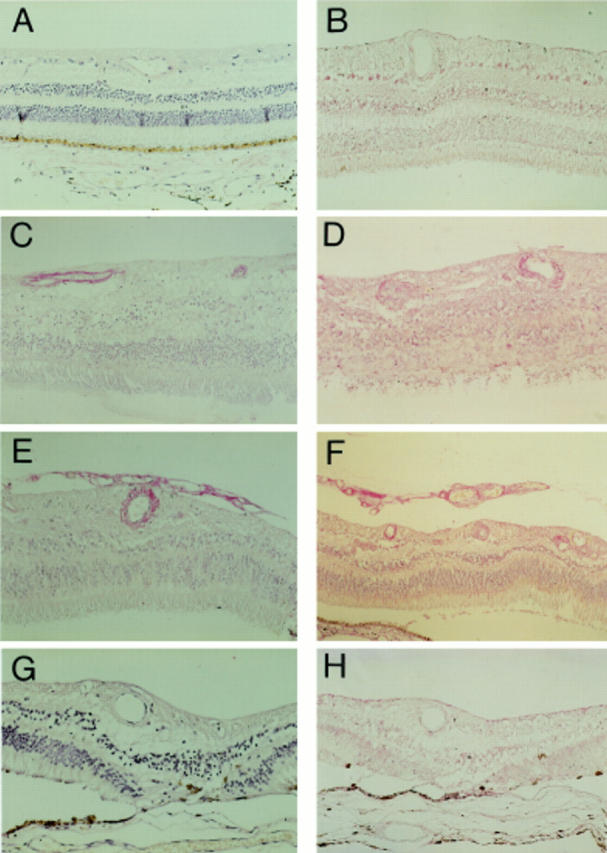
Methods: Immunohistochemical localisation of VEGF, using antibodies raised against VEGF165 and VEGF121,165,189, was carried out on specimens of normal human retina (n = 15), diabetic retinas ((a) with no overt retinopathy (n = 19), (b) with intraretinal vascular abnormalities but no proliferative retinopathy (n = 6), (c) with active proliferative retinopathy (n = 6), (d) with no residual proliferative retinopathy after photocoagulation therapy (n = 15)), excised diabetic fibrovascular membranes (n = 19), and non-diabetic fibrocellular membranes (n = 7). The degree and pattern of immunostaining was recorded.
Results: In general, VEGF was absent from the majority of normal retinas. VEGF staining was apparent in most diabetic tissues but the staining pattern was dependent on both the specificity of the antibody used and the category of tissue. Staining with the VEGF165 antibody was generally confined to endothelial cells adn perivascular regions while the VEGF121,165,189 antibody was also associated with extravascular components of the inner retina. Intensity of immunostaining of diabetic eyes was dependent on the severity of retinopathy being least in diabetics with no overt retinopathy and greatest in retinas with proliferative retinopathy. Interestingly, the intensity of immunostaining in diabetic retinas which had undergone laser surgery for proliferative retinopathy was reduced to basal levels. Moderate to intense immunostaining was observed in all fibrovascular and fibrocellular membranes examined.
Conclusions: This study supports a circumstantial role for VEGF in the pathogenesis of both the preclinical and proliferative stages of diabetic retinopathy.
Figures
Similar articles
-
Immunolocalisation of the VEGF receptors FLT-1, KDR, and FLT-4 in diabetic retinopathy.Br J Ophthalmol. 1999 Apr;83(4):486-94. doi: 10.1136/bjo.83.4.486. Br J Ophthalmol. 1999. PMID: 10434875 Free PMC article.
-
Increased expression of placenta growth factor in proliferative diabetic retinopathy.Lab Invest. 1998 Jan;78(1):109-16. Lab Invest. 1998. PMID: 9461127
-
Vascular endothelial growth factor is present in glial cells of the retina and optic nerve of human subjects with nonproliferative diabetic retinopathy.Invest Ophthalmol Vis Sci. 1997 Jan;38(1):36-47. Invest Ophthalmol Vis Sci. 1997. PMID: 9008628
-
[Cell biology of intraocular vascular diseases].Nippon Ganka Gakkai Zasshi. 1999 Dec;103(12):923-47. Nippon Ganka Gakkai Zasshi. 1999. PMID: 10643294 Review. Japanese.
-
[Effective mechanisms of laser photocoagulation for neovascularization in diabetic retinopathy].Nippon Ganka Gakkai Zasshi. 1996 May;100(5):339-49. Nippon Ganka Gakkai Zasshi. 1996. PMID: 8651051 Review. Japanese.
Cited by
-
sFlt Multivalent Conjugates Inhibit Angiogenesis and Improve Half-Life In Vivo.PLoS One. 2016 Jun 3;11(6):e0155990. doi: 10.1371/journal.pone.0155990. eCollection 2016. PLoS One. 2016. PMID: 27257918 Free PMC article.
-
Diabetic Retinopathy in Patients with Diabetic Nephropathy: Development and Progression.PLoS One. 2016 Aug 26;11(8):e0161897. doi: 10.1371/journal.pone.0161897. eCollection 2016. PLoS One. 2016. PMID: 27564383 Free PMC article.
-
Multivalent hyaluronic acid bioconjugates improve sFlt-1 activity in vitro.Biomaterials. 2016 Jul;93:95-105. doi: 10.1016/j.biomaterials.2016.03.017. Epub 2016 Mar 12. Biomaterials. 2016. PMID: 27086270 Free PMC article.
-
Vulnerability of the developing brain to hypoxic-ischemic damage: contribution of the cerebral vasculature to injury and repair?Front Physiol. 2012 Nov 9;3:424. doi: 10.3389/fphys.2012.00424. eCollection 2012. Front Physiol. 2012. PMID: 23162470 Free PMC article.
-
ERK5 Mediated Signalling in Diabetic Retinopathy.Med Hypothesis Discov Innov Ophthalmol. 2015 Spring;4(1):17-26. Med Hypothesis Discov Innov Ophthalmol. 2015. PMID: 25861671 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous