

Investigation by Parkinson's Disease Research Group of United Kingdom into excess mortality seen with combined levodopa and selegiline treatment in patients with early, mild Parkinson's disease: further results of randomised trial and confidential inquiry
- PMID: 9583926
- PMCID: PMC28519
- DOI: 10.1136/bmj.316.7139.1191
Investigation by Parkinson's Disease Research Group of United Kingdom into excess mortality seen with combined levodopa and selegiline treatment in patients with early, mild Parkinson's disease: further results of randomised trial and confidential inquiry
Abstract
Objective: To determine whether the excess mortality observed in patients who received both levodopa and selegiline in a randomised trial could be explained by revised diagnosis of Parkinson's disease, autonomic or cardiovascular effects, more rapid disease progression, or drug interactions.
Design: Open randomised trial and blind comparison and reclassification of the cause of death of patients who were recruited from 93 hospitals between 1985 and 1990 and who had died before December 1993 in arms 1 and 2.
Setting: United Kingdom.
Subjects: 624 patients with early Parkinson's disease who were not receiving dopaminergic treatment and a subgroup fo 120 patients who died during the trial.
Interventions: Levodopa and a dopa carboxylase inhibitor (arm 1), levodopa and a dopa decarboxylase inhibitor in combination with selegiline (arm 2), or bromocriptine alone (arm 3).
Main outcome measures: All cause mortality for 520 subjects in arms 1 and 2 and for 104 subjects who were randomised into these arms from arm 3. Cause specific mortality for people who died in the original arms 1 and 2 on the basis of the opinion of a panel, revised diagnosis and disability ratings, evidence from clinical records of either autonomic or cardiovascular episodes, other clinical features before death, and drug interactions.
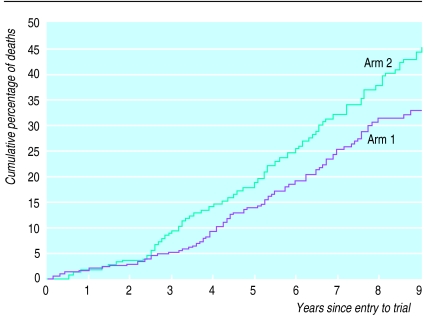
Results: After extended follow up (mean 6.8 years) until the end of September 1995, when arm 2 was terminated, the hazard ratio for arm 2 compared with arm 1 was 1.32 (95% confidence interval 0.98 to 1.79). For subjects who were randomised from arm 3 the hazard ratio for arm 2 was 1.54 (0.83 to 2.87). When all subjects were included the hazard ratio was 1.33 (1.02 to 1.74) and after adjustment for other baseline factors it was 1.30 (0.99 to 1.72). The excess mortality seemed to be greatest in the third and fourth year of follow up. Cause specific death rates showed an excess of deaths from Parkinson's disease only (hazard ratio 2.5 (1.3 to 4.7)). No significant differences were found for revised diagnosis, disability rating scores, autonomic or cardiovascular events, other clinical features, or drug interactions. Patients who died in arm 2 were more likely to have had possible dementia and a history of falls before death compared with those who died in arm 1.
Conclusion: The results consistently show excess mortality in patients treated with combined levodopa and selegiline. Revised diagnosis, autonomic or cardiovascular events, or drug interactions could not explain this finding, but falls and possible dementia were more common in arm 2. The results do not support combined treatment in patients with newly diagnosed Parkinson's disease. In more advanced disease, combined treatment should perhaps be avoided in patients with postural hypotension, frequent falls, confusion, or dementia.
Figures
Comment in
-
Selegiline, or the problem of early termination of clinical trials. The clinical questions are not well answered, and probably never will be.BMJ. 1998 Apr 18;316(7139):1182-3. doi: 10.1136/bmj.316.7139.1182. BMJ. 1998. PMID: 9552992 Free PMC article. No abstract available.
-
Monitoring randomised controlled trials. Parkinson's disease trial illustrates the dangers of stopping early.BMJ. 1998 Apr 18;316(7139):1183-4. doi: 10.1136/bmj.316.7139.1183. BMJ. 1998. PMID: 9552993 Free PMC article. No abstract available.
-
Effect of adding selegiline to levodopa in early, mild Parkinson's disease. Formal systematic review of data on patients in all relevant trials is required.BMJ. 1998 Dec 5;317(7172):1586. BMJ. 1998. PMID: 9836669 Free PMC article. No abstract available.
-
Effect of adding selegiline to levodopa in early, mild Parkinson's disease. Evidence is insufficient to show that combined treatment increases mortality.BMJ. 1998 Dec 5;317(7172):1586-7. BMJ. 1998. PMID: 9890764 No abstract available.
Similar articles
-
Comparison of therapeutic effects and mortality data of levodopa and levodopa combined with selegiline in patients with early, mild Parkinson's disease. Parkinson's Disease Research Group of the United Kingdom.BMJ. 1995 Dec 16;311(7020):1602-7. doi: 10.1136/bmj.311.7020.1602. BMJ. 1995. PMID: 8555803 Free PMC article. Clinical Trial.
-
Comparisons of therapeutic effects of levodopa, levodopa and selegiline, and bromocriptine in patients with early, mild Parkinson's disease: three year interim report. Parkinson's Disease Research Group in the United Kingdom.BMJ. 1993 Aug 21;307(6902):469-72. doi: 10.1136/bmj.307.6902.469. BMJ. 1993. PMID: 8400928 Free PMC article. Clinical Trial.
-
Ten-year follow-up of three different initial treatments in de-novo PD: a randomized trial.Neurology. 2001 Nov 13;57(9):1687-94. doi: 10.1212/wnl.57.9.1687. Neurology. 2001. PMID: 11706112 Clinical Trial.
-
Strategies in the treatment of early Parkinson's disease.Acta Neurol Scand Suppl. 1993;146:50-3. Acta Neurol Scand Suppl. 1993. PMID: 8101417 Review.
-
Safety of selegiline (deprenyl) in the treatment of Parkinson's disease.Drug Saf. 1998 Jul;19(1):11-22. doi: 10.2165/00002018-199819010-00002. Drug Saf. 1998. PMID: 9673855 Review.
Cited by
-
Inhibitors of MAO-A and MAO-B in Psychiatry and Neurology.Front Pharmacol. 2016 Oct 18;7:340. doi: 10.3389/fphar.2016.00340. eCollection 2016. Front Pharmacol. 2016. PMID: 27803666 Free PMC article. Review.
-
Using monoamine oxidase type B inhibitors in Parkinson's disease.BMJ. 2004 Sep 11;329(7466):581-2. doi: 10.1136/bmj.329.7466.581. BMJ. 2004. PMID: 15361418 Free PMC article. No abstract available.
-
Issues for clinical drug development in neurodegenerative diseases.Drugs. 2005;65(17):2463-79. doi: 10.2165/00003495-200565170-00004. Drugs. 2005. PMID: 16296872 Review.
-
Monoamine oxidase B inhibitors for early Parkinson's disease.Cochrane Database Syst Rev. 2005 Jul 20;2005(3):CD004898. doi: 10.1002/14651858.CD004898.pub2. Cochrane Database Syst Rev. 2005. PMID: 16034956 Free PMC article. Review.
-
Cost utility of drugs for multiple sclerosis. Systematic review places study in contrast.BMJ. 2000 May 27;320(7247):1474-5; author reply 1475-6. BMJ. 2000. PMID: 10877569 Free PMC article. No abstract available.
References
-
- Tatton WG, Greenwood CE. Rescue of dying neurones: a new action for deprenyl in MPTP parkinsonism. J Neurol Sci. 1991;30:666–672. - PubMed
-
- Parkinson Study Group. Effect of deprenyl on the progression of disability in early Parkinson’s disease. N Engl J Med. 1989;321:1364–1371. - PubMed
-
- Birkmayer W, Knoll J, Riederer P, Youdim MBH, Hars V, Marton J. Increased life expectancy resulting from addition of l-deprenyl to Madopar treatment in Parkinson’s disease: a long-term study. J Neural Transm. 1985;64:113–127. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical