

Antibody-mediated protection against respiratory syncytial virus in children
- PMID: 39384305
- PMCID: PMC11462297
- DOI: 10.1183/16000617.0106-2024
Antibody-mediated protection against respiratory syncytial virus in children
Abstract
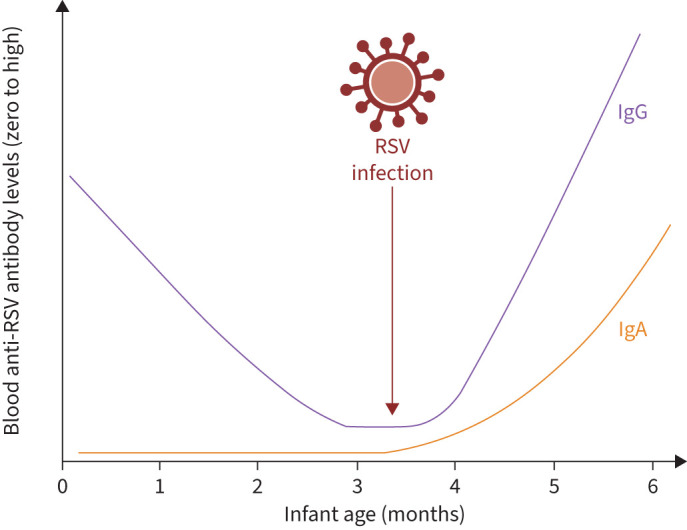
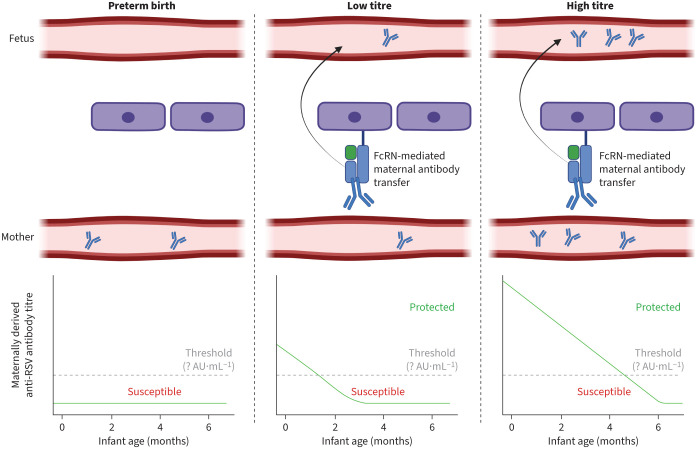
Respiratory syncytial virus (RSV) is a major global pathogen, causing lower respiratory tract disease in at-risk populations including young children. Antibodies form a crucial layer of protection from RSV disease, particularly in immunologically naïve infants. Such antibodies are derived from the mother via transplacental transfer and breast milk, but may be particularly low in high-risk infants such as those born preterm. Maternally derived antibodies can now be supplemented by the administration of anti-RSV monoclonal antibodies, while a rising wave of maternal and paediatric vaccine strategies are approaching. The implementation of these prophylactics may profoundly decrease the healthcare burden of RSV. In this article, we review the role of antibody-mediated immunity in protecting children from RSV. We focus on maternally derived antibodies as the main source of protection against RSV and study factors that influence the scale of this transfer. The role of passive and active prophylactic approaches in protecting infants against RSV are discussed and knowledge gaps in our understanding of antibody-mediated protection against RSV are identified.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: A. Moureau is an employee of Sanofi and owns Sanofi stock as an employee. C. Vernhes was an employee of Sanofi at the time the work was performed, owns Sanofi stock as a former employee and is currently employed by the trade association Vaccines Europe. P.J.M. Openshaw reports consulting fees from GSK, Moderna, Janssen, Seqirus, Pfizer, Sanofi, AstraZeneca, and Icosavax; honoraria for lectures from GSK, Moderna, Seqirus, Sanofi, and AstraZeneca; participation on a Data Safety Monitoring Board for Sanofi; board membership for the Science Media Centre and a role as governor for Sidcot School. R.S. Thwaites reports consulting fees from AOBiome, Gossamer Bio, Indalo Therapeutics, and PrEP Biopharm; and honoraria for lectures from AstraZeneca and GSK. All other authors report no conflicts of interest.
Figures
Similar articles
-
Passive Immunization Strategies to Prevent Severe Respiratory Syncytial Virus Infection Among Newborns and Young Infants.J Pediatric Infect Dis Soc. 2024 Jul 12;13(Supplement_2):S110-S114. doi: 10.1093/jpids/piae058. J Pediatric Infect Dis Soc. 2024. PMID: 38995085 Review.
-
Transplacental transfer of maternal respiratory syncytial virus (RSV) antibody and protection against RSV disease in infants in rural Nepal.J Clin Virol. 2017 Oct;95:90-95. doi: 10.1016/j.jcv.2017.08.017. Epub 2017 Sep 2. J Clin Virol. 2017. PMID: 28903080 Free PMC article.
-
New and Emerging Passive Immunization Strategies for the Prevention of RSV Infection During Infancy.J Pediatric Infect Dis Soc. 2024 Jul 12;13(Supplement_2):S115-S124. doi: 10.1093/jpids/piae030. J Pediatric Infect Dis Soc. 2024. PMID: 38554101 Review.
-
Alternative Virus-Like Particle-Associated Prefusion F Proteins as Maternal Vaccines for Respiratory Syncytial Virus.J Virol. 2019 Nov 13;93(23):e00914-19. doi: 10.1128/JVI.00914-19. Print 2019 Dec 1. J Virol. 2019. PMID: 31511382 Free PMC article.
-
Respiratory syncytial virus in infants: is maternal vaccination a realistic strategy?Curr Opin Infect Dis. 2015 Jun;28(3):221-4. doi: 10.1097/QCO.0000000000000161. Curr Opin Infect Dis. 2015. PMID: 25918956 Review.
References
-
- Shi T, McAllister DA, O'Brien KL, et al. . Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet 2017; 390: 946–958. doi:10.1016/S0140-6736(17)30938-8 - DOI - PMC - PubMed
-
- Li Y, Wang X, Blau DM, et al. . Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet 2022; 399: 2047–2064. doi:10.1016/S0140-6736(22)00478-0 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical