

A Cost-Utility Analysis of the Use of -125 mm Hg Closed-incision Negative Pressure Therapy in Oncoplastic Breast Surgery
- PMID: 39359700
- PMCID: PMC11444648
- DOI: 10.1097/GOX.0000000000006163
A Cost-Utility Analysis of the Use of -125 mm Hg Closed-incision Negative Pressure Therapy in Oncoplastic Breast Surgery
Abstract
Background: Closed-incision negative pressure therapy (ciNPT) decreases the rate of wound complications in oncoplastic breast surgery (OBS) but at a fiscal cost. Our aim was to examine the cost-utility of ciNPT in OBS.
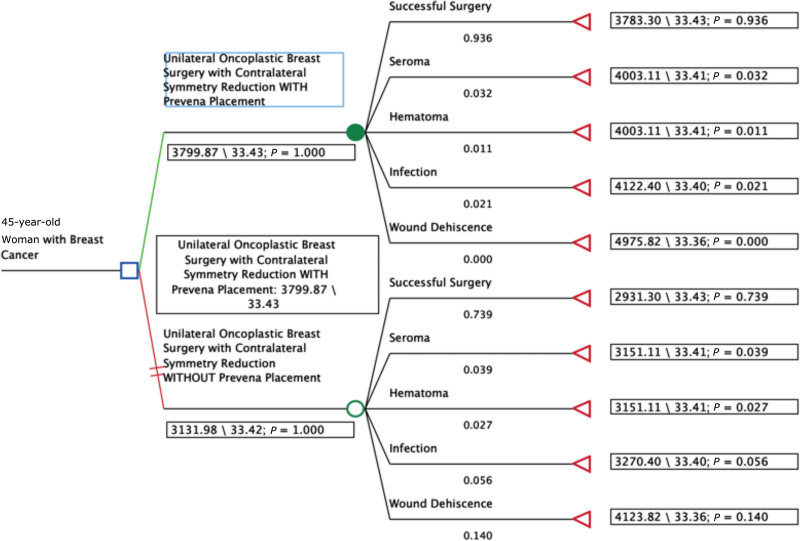
Methods: A literature review was performed to obtain the probabilities and outcomes for the treatment of unilateral breast cancer with OBS with ciNPT versus without. Reported utility scores in the literature were used to calculate quality-adjusted life years (QALYs) for each health state. A decision analysis tree was constructed with rollback analysis to determine the more cost-effective strategy. An incremental cost-utility ratio was calculated. Sensitivity analyses were performed.
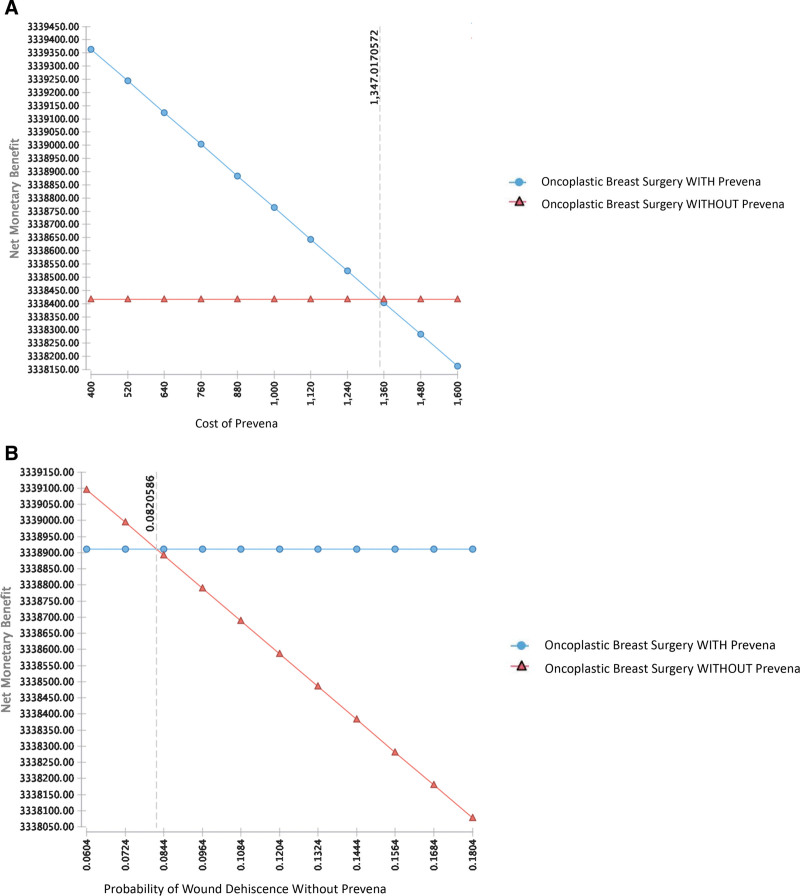
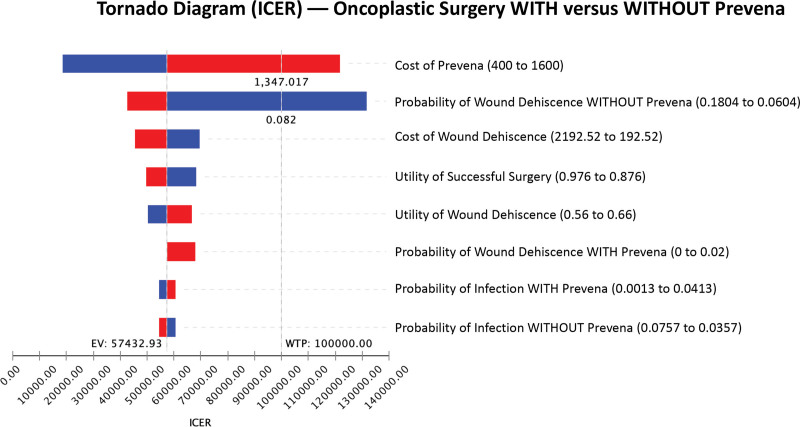
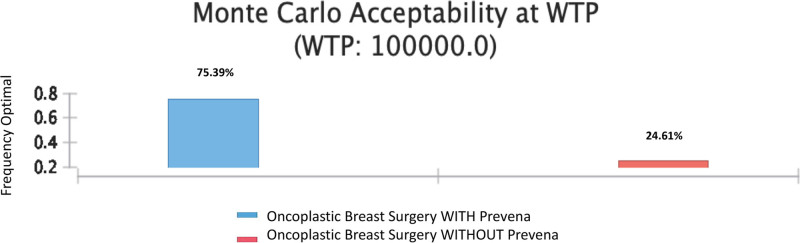
Results: OBS with ciNPT is associated with a higher clinical effectiveness (QALY) of 33.43 compared to without (33.42), and relative cost increase of $667.89. The resulting incremental cost-utility ratio of $57432.93/QALY favored ciNPT. In one-way sensitivity analysis, ciNPT was the more cost-effective strategy if the cost of ciNPT was less than $1347.02 or if the probability of wound dehiscence without was greater than 8.2%. Monte Carlo analysis showed a confidence of 75.39% that surgery with ciNPT is more cost effective.
Conclusion: Despite the added cost, surgery with ciNPT is cost-effective. This finding is a direct result of decreased overall wound complications with ciNPT.
Copyright © 2024 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
Dr. Chatterjee is a consultant for 3M and DeRoyal. All the other authors have no financial interest to declare in relation to the content of this article.
Figures
Similar articles
-
A Cost-Utility Analysis of the Use of Closed-Incision Negative Pressure System in Vascular Surgery Groin Incisions.Am Surg. 2023 Jun;89(6):2237-2246. doi: 10.1177/00031348221087395. Epub 2022 Apr 7. Am Surg. 2023. PMID: 35392664 Review.
-
A Cost-Utility Analysis Comparing Immediate Oncoplastic Surgery with Delayed Oncoplastic Surgery in Smoking Breast Cancer Patients.Ann Surg Oncol. 2021 May;28(5):2579-2588. doi: 10.1245/s10434-020-09220-z. Epub 2020 Oct 13. Ann Surg Oncol. 2021. PMID: 33051741
-
Closed Incision Negative Pressure Therapy in Oncoplastic Breast Surgery: A Comparison of Outcomes.Plast Reconstr Surg Glob Open. 2023 Apr 25;11(4):e4936. doi: 10.1097/GOX.0000000000004936. eCollection 2023 Apr. Plast Reconstr Surg Glob Open. 2023. PMID: 37113306 Free PMC article.
-
Closed Incision Negative Pressure Therapy in Oncoplastic Surgery Prevents Delays to Adjuvant Therapy.Plast Reconstr Surg Glob Open. 2023 May 26;11(5):e5028. doi: 10.1097/GOX.0000000000005028. eCollection 2023 May. Plast Reconstr Surg Glob Open. 2023. PMID: 37250834 Free PMC article.
-
Closed Incision Negative Pressure Therapy vs Standard of Care Dressing in Breast Surgery: A Systematic Review.Cureus. 2022 Apr 26;14(4):e24499. doi: 10.7759/cureus.24499. eCollection 2022 Apr. Cureus. 2022. PMID: 35651408 Free PMC article. Review.
References
-
- Chatterjee A, Pyfer B, Czerniecki B, et al. . Early postoperative outcomes in lumpectomy versus simple mastectomy. J Surg Res. 2015;198:143–148. - PubMed
-
- Chatterjee A, Gass J, Patel K, et al. . A consensus definition and classification system of oncoplastic surgery developed by the American Society of Breast Surgeons. Ann Surg Oncol. 2019;26:3436–3444. - PubMed
-
- Losken A, Chatterjee A. Improving results in oncoplastic surgery. Plast Reconstr Surg. 2021;147:123e–134e. - PubMed
LinkOut - more resources
Full Text Sources