

Respiratory Viral Testing Rate Patterns in Young Children Attending Tertiary Care Across Western Australia: A Population-Based Birth Cohort Study
- PMID: 39225070
- PMCID: PMC11369639
- DOI: 10.1111/irv.70005
Respiratory Viral Testing Rate Patterns in Young Children Attending Tertiary Care Across Western Australia: A Population-Based Birth Cohort Study
Abstract
Background: An understanding of viral testing rates is crucial to accurately estimate the pathogen-specific hospitalisation burden. We aimed to estimate the patterns of testing for respiratory syncytial virus (RSV), influenza virus, parainfluenza virus (PIV) and human metapneumovirus (hMPV) by geographical location, age and time in children <5 years old in Western Australia.
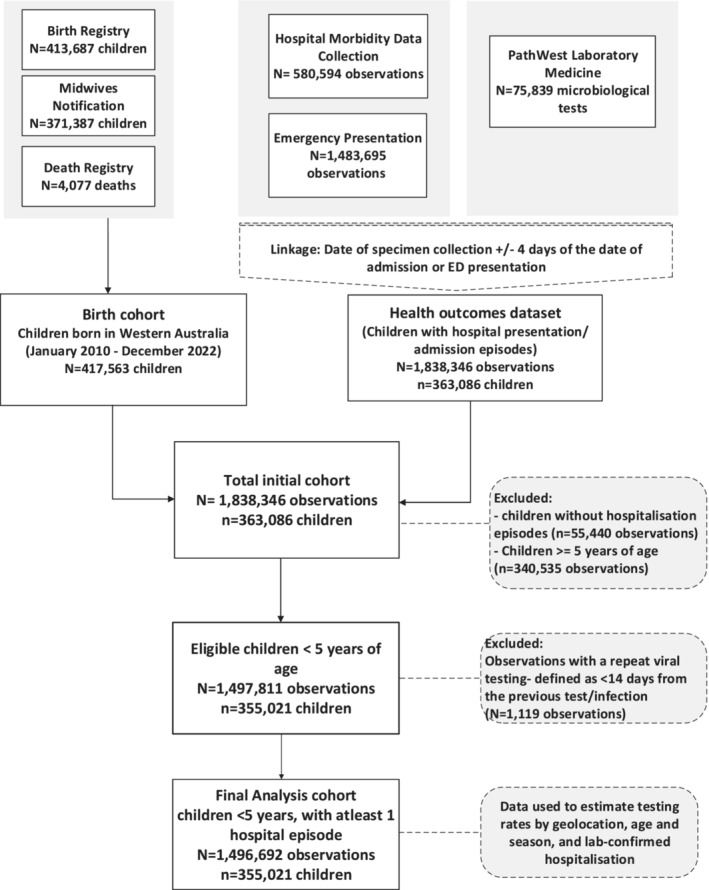
Methods: We conducted a population-based cohort study of children born between 1 January 2010 and 31 December 2021, utilising linked administrative data incorporating birth and death records, hospitalisations and respiratory viral surveillance testing records from state-wide public pathology data. We examined within-hospital testing rates using survival analysis techniques and identified independent predictors of testing using binary logistic regression.
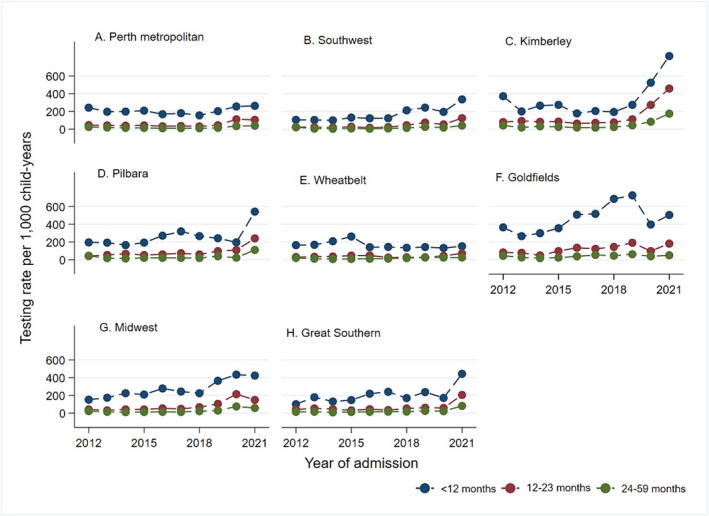
Results: Our dataset included 46,553 laboratory tests for RSV, influenza, PIV, or hMPV from 355,021 children (52.5% male). Testing rates declined in the metropolitan region over the study period (RSV testing in infants: from 242.11/1000 child-years in 2012 to 155.47/1000 child-years in 2018) and increased thereafter. Conversely, rates increased in non-metropolitan areas (e.g., RSV in Goldfields: from 364.92 in 2012 to 504.37/1000 child-years in 2021). The strongest predictors of testing were age <12 months (adjusted odds ratio [aOR] = 2.25, 95% CI 2.20-2.31), preterm birth (<32 weeks: aOR = 2.90, 95% CI 2.76-3.05) and remote residence (aOR = 0.77, 95% CI 0.73-0.81).
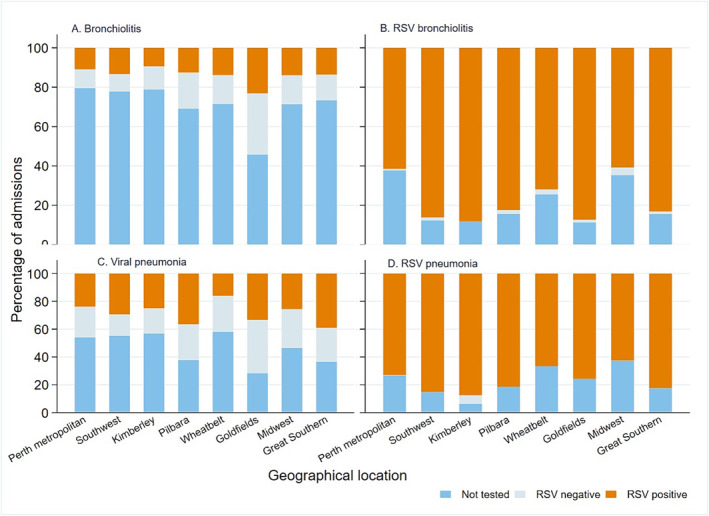
Conclusion: These current testing rates highlight the potential underestimation of respiratory virus hospitalisations by routine surveillance and the need for estimation of the true burden of respiratory virus admissions.
Keywords: Australia; geographic variation; respiratory virus; within‐hospital laboratory testing.
© 2024 The Author(s). Influenza and Other Respiratory Viruses published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Record linkage study of the pathogen-specific burden of respiratory viruses in children.Influenza Other Respir Viruses. 2017 Nov;11(6):502-510. doi: 10.1111/irv.12508. Epub 2017 Oct 30. Influenza Other Respir Viruses. 2017. PMID: 28991397 Free PMC article.
-
Severe acute respiratory infection in children in a densely populated urban slum in Kenya, 2007-2011.BMC Infect Dis. 2015 Feb 25;15:95. doi: 10.1186/s12879-015-0827-x. BMC Infect Dis. 2015. PMID: 25879805 Free PMC article.
-
Characteristics of human metapneumovirus infection in adults hospitalized for community-acquired influenza-like illness in France, 2012-2018: a retrospective observational study.Clin Microbiol Infect. 2021 Jan;27(1):127.e1-127.e6. doi: 10.1016/j.cmi.2020.04.005. Epub 2020 Apr 10. Clin Microbiol Infect. 2021. PMID: 32283266 Free PMC article.
-
Children with respiratory disease associated with metapneumovirus in Hong Kong.Emerg Infect Dis. 2003 Jun;9(6):628-33. doi: 10.3201/eid0906.030009. Emerg Infect Dis. 2003. PMID: 12781000 Free PMC article.
-
Clinical impact and diagnosis of human metapneumovirus infection.Pediatr Infect Dis J. 2004 Jan;23(1 Suppl):S25-32. doi: 10.1097/01.inf.0000108190.09824.e8. Pediatr Infect Dis J. 2004. PMID: 14730267 Review.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
