

A mouldable fibreglass backslab device as a novel approach to offload chronic plantar foot ulcers: A retrospective observational audit
- PMID: 39169647
- PMCID: PMC11339119
- DOI: 10.1002/jfa2.70001
A mouldable fibreglass backslab device as a novel approach to offload chronic plantar foot ulcers: A retrospective observational audit
Abstract
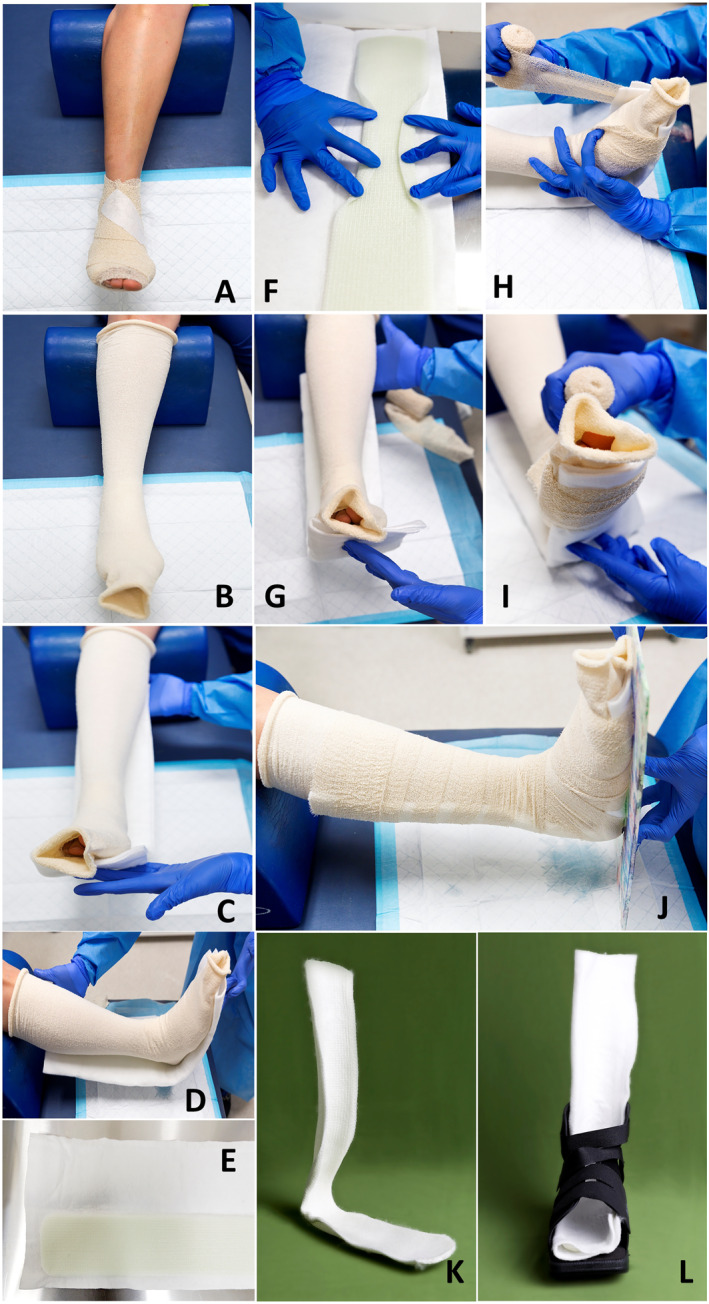
Background: Pressure offloading is a critical component of plantar foot ulcer management, including diabetes-related foot ulcers (DFU). Conventional offloading options such as total contact casting and removable knee-high walkers may be unsuitable or unsuccessful in patients with morbid obesity, intermittent lower limb oedema, high exudative wounds or poor mobility. A mouldable fibreglass backslab device (BSD) may be a practical alternative to be considered in these situations.
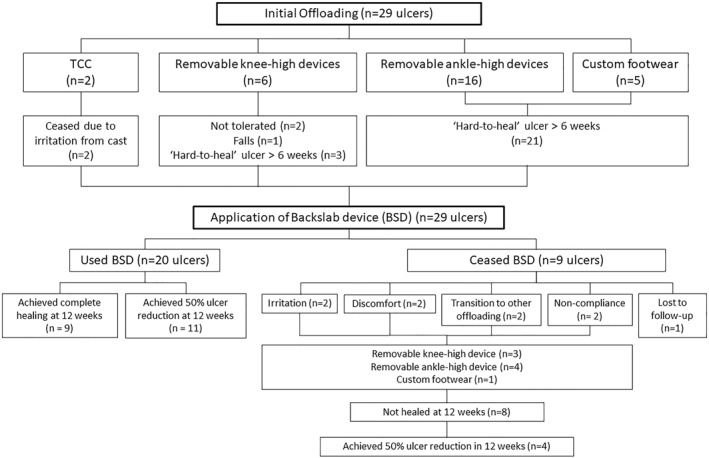
Methods: Data were retrospectively collected on 28 patients (29 foot ulcers) with non-healing ulcers who received a BSD to offload their foot ulcer as an extension to standard offloading care. Baseline data included: patient demographics, type of offloading prior to BSD application, date of ulcer onset, days ulcer present prior to BSD application and ulcer size at BSD initiation. Measures of success included ulcer size reduction 12 weeks post-BSD application, time to complete ulcer healing in BSD, time to 50% reduction in ulcer size post-BSD application and total number of days ulcer present.
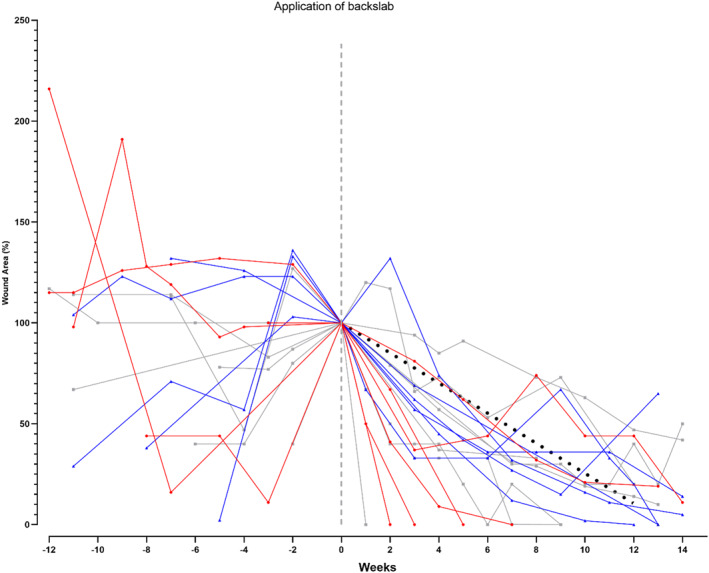
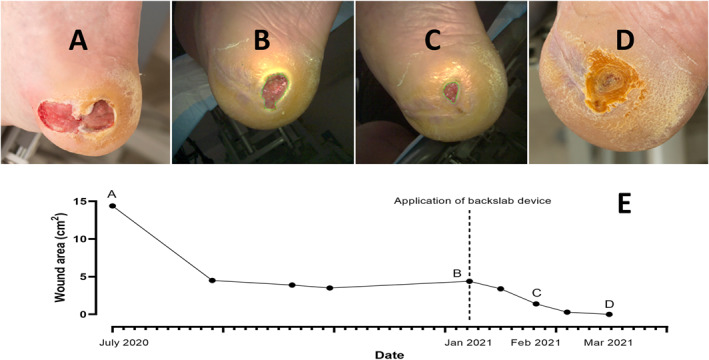
Results: The median (IQR) ulcer area and ulcer duration at baseline for 19 patients (20 ulcers) who used the BSD was 1.65 (0.4-3.8) cm2 and 531 (101-635) days. At 12 weeks, the median (IQR) ulcer area was 0.3 (0-0.55) cm2 with a median (IQR) reduction of 97 (80-100) %. Nine (45%) ulcers achieved complete wound healing (100% reduction in wound size) at 12 weeks post-BSD application, and the remaining 11 (55%) ulcers achieved at least 50% reduction in wound size. The median (IQR) time to complete wound healing and 50% reduction in wound size was 71 (35-134) days and 24 (15-44) days, respectively. Nine patients ceased use of the BSD and reverted to conventional offloading before their wounds had healed. Of these, four patients achieved a 50% reduction in wound size at the 12-week mark with conventional offloading.
Conclusion: Our preliminary data suggests that a mouldable fibreglass BSD may be a practical offloading option in the management of DFUs, especially when conventional offloading methods are unsuccessful, unsuitable or unacceptable to patients. Higher level evidence is required to demonstrate suitability or efficacy of the BSD compared to current evidence-based recommended offloading methods.
Keywords: diabetic foot; foot ulcer; offloading; retrospective studies; ulcer healing.
© 2024 The Author(s). Journal of Foot and Ankle Research published by John Wiley & Sons Australia, Ltd on behalf of Australian Podiatry Association and The Royal College of Podiatry.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Australian guideline on offloading treatment for foot ulcers: part of the 2021 Australian evidence-based guidelines for diabetes-related foot disease.J Foot Ankle Res. 2022 May 5;15(1):31. doi: 10.1186/s13047-022-00538-3. J Foot Ankle Res. 2022. PMID: 35513821 Free PMC article.
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Defining the optimum strategy for identifying adults and children with coeliac disease: systematic review and economic modelling.Health Technol Assess. 2022 Oct;26(44):1-310. doi: 10.3310/ZUCE8371. Health Technol Assess. 2022. PMID: 36321689 Free PMC article.
-
Therapeutic ultrasound for venous leg ulcers.Cochrane Database Syst Rev. 2017 May 15;5(5):CD001180. doi: 10.1002/14651858.CD001180.pub4. Cochrane Database Syst Rev. 2017. PMID: 28504325 Free PMC article. Review.
-
Phototherapy for treating pressure ulcers.Cochrane Database Syst Rev. 2014 Jul 11;2014(7):CD009224. doi: 10.1002/14651858.CD009224.pub2. Cochrane Database Syst Rev. 2014. PMID: 25019295 Free PMC article. Review.
References
-
- Lazzarini, P. A. , Jarl G., Gooday C., Viswanathan V., Caravaggi C. F., Armstrong D. G., and Bus S. A.. 2020. “Effectiveness of Offloading Interventions to Heal Foot Ulcers in Persons with Diabetes: A Systematic Review.” Diabetes/Metabolism Research and Reviews 36(S1): e3275–n/a. 10.1002/dmrr.3275. - DOI - PMC - PubMed
-
- Bhatt, U. K. , Foo H. Y., McEvoy M. P., Tomlinson S. J., Westphal C., Harrison J. C., Oshin O., and Carter S. L.. 2021. “Is TCC‐EZ a Suitable Alternative to Gold Standard Total‐Contact Casting? A Plantar Pressure Analysis.” Journal of the American Podiatric Medical Association 111(5): 1. 10.7547/8750-7315-111-5.article_1. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
