

Current Landscape and Future Directions of Coronary Revascularization in Ischemic Systolic Heart Failure: A Review
- PMID: 39131064
- PMCID: PMC11307589
- DOI: 10.1016/j.jscai.2023.101197
Current Landscape and Future Directions of Coronary Revascularization in Ischemic Systolic Heart Failure: A Review
Abstract
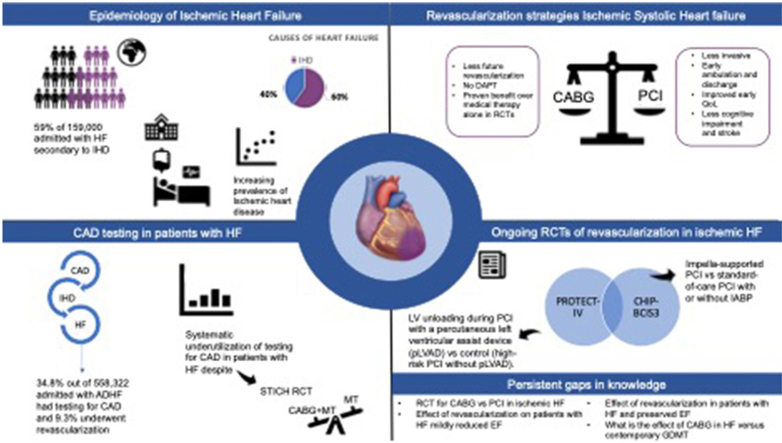
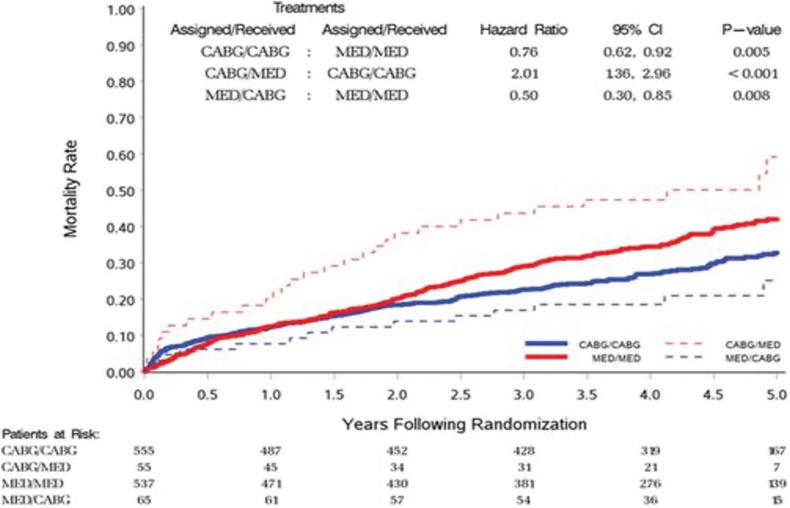
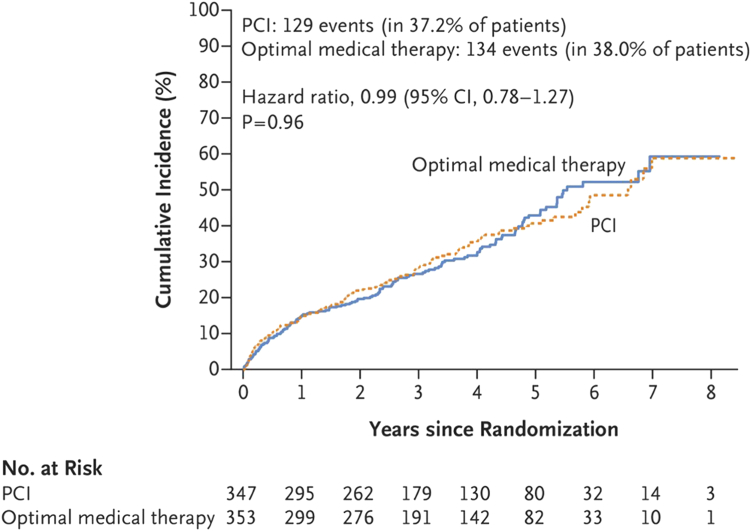
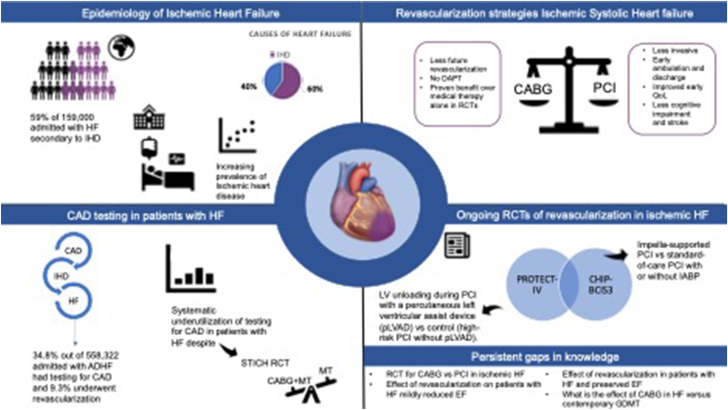
Ischemic heart disease is the largest cause of death worldwide and the most common cause of heart failure (HF). The incidence and prevalence of HF are increasing owing to an aging population and improvements in the acute cardiac care of previously fatal conditions such as myocardial infarction. Strategies to improve outcomes in patients with ischemic systolic HF are urgently needed. There is systematic underutilization of testing for coronary artery disease in patients with HF, and revascularization is performed in an even smaller minority despite evidence for reduced mortality with coronary artery bypass grafting (CABG) over medical therapy in the Surgical Treatment for Ischemic Heart Failure Extension Study. Percutaneous coronary intervention (PCI) is a less-invasive approach to coronary revascularization; however, the recent Revascularization for Ischemic Ventricular Dysfunction (REVIVED)-British Cardiovascular Intervention Society (BCIS2) trial failed to demonstrate a benefit of PCI compared with that of medical therapy in patients with ischemic systolic HF. The comparative effectiveness of PCI and CABG for patients with ischemic systolic HF remains unknown, particularly in the era of contemporary medical therapy. In this review, we discuss the benefit of CABG in ischemic systolic HF, its underutilization, and the unmet clinical need. We also review the recent REVIVED-BCIS2 trial comparing PCI to medical therapy, as well as upcoming randomized controlled trials of PCI for ischemic systolic HF and persistent evidence gaps that will exist despite anticipated data from ongoing trials. There remains a need for an adequately powered randomized controlled trials to establish the comparative clinical effectiveness of PCI vs CABG in ischemic systolic HF in the era of contemporary revascularization approaches and medical therapy, as well as trials of coronary revascularization in patients with HF with preserved ejection fraction or less severe forms of left ventricular systolic dysfunction.
Keywords: heart failure; percutaneous coronary intervention; revascularization.
© 2023 Published by Elsevier Inc. on behalf of the Society for Cardiovascular Angiography and Interventions Foundation.
Figures


Similar articles
-
Percutaneous Revascularization for Ischemic Ventricular Dysfunction: Rationale and Design of the REVIVED-BCIS2 Trial: Percutaneous Coronary Intervention for Ischemic Cardiomyopathy.JACC Heart Fail. 2018 Jun;6(6):517-526. doi: 10.1016/j.jchf.2018.01.024. JACC Heart Fail. 2018. PMID: 29852933
-
PCI in Patients With Heart Failure: Current Evidence, Impact of Complete Revascularization, and Contemporary Techniques to Improve Outcomes.J Soc Cardiovasc Angiogr Interv. 2022 Apr 11;1(2):100020. doi: 10.1016/j.jscai.2022.100020. eCollection 2022 Mar-Apr. J Soc Cardiovasc Angiogr Interv. 2022. PMID: 39132568 Free PMC article. Review.
-
Enhanced External Counterpulsation (EECP): An Evidence-Based Analysis.Ont Health Technol Assess Ser. 2006;6(5):1-70. Epub 2006 Mar 1. Ont Health Technol Assess Ser. 2006. PMID: 23074496 Free PMC article.
-
Percutaneous Revascularization for Ischemic Left Ventricular Dysfunction: Cost-Effectiveness Analysis of the REVIVED-BCIS2 Trial.Circ Cardiovasc Qual Outcomes. 2024 Jan;17(1):e010533. doi: 10.1161/CIRCOUTCOMES.123.010533. Epub 2023 Nov 6. Circ Cardiovasc Qual Outcomes. 2024. PMID: 37929587 Free PMC article. Clinical Trial.
-
Outcomes of Percutaneous Revascularization in Severe Ischemic Left Ventricular Dysfunction.Curr Cardiol Rep. 2024 May;26(5):435-442. doi: 10.1007/s11886-024-02045-2. Epub 2024 Apr 20. Curr Cardiol Rep. 2024. PMID: 38642298 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
