

Glycemic Burden and Clinical Outcomes of Early Stage Hepatocellular Carcinoma after Curative Treatment
- PMID: 39123380
- PMCID: PMC11311804
- DOI: 10.3390/cancers16152652
Glycemic Burden and Clinical Outcomes of Early Stage Hepatocellular Carcinoma after Curative Treatment
Abstract
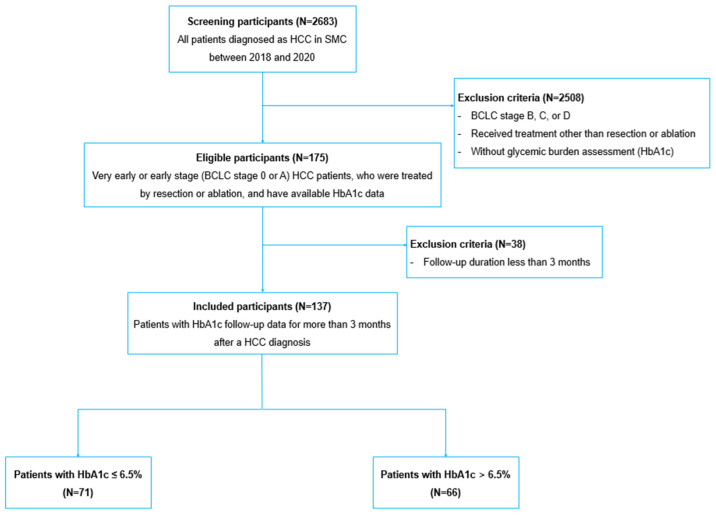
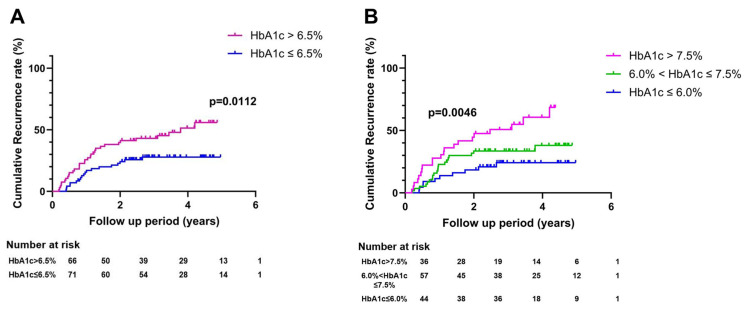
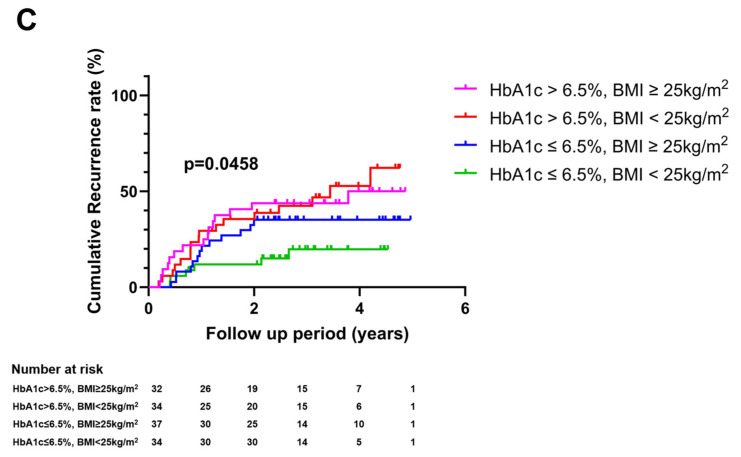
Early-stage hepatocellular carcinoma (HCC) is still difficult to cure for its high recurrence rate. This study aimed to examine whether glycemic burden management could be one way to improve outcomes of early-stage HCC. A total of 137 very early or early-stage HCC patients who underwent resection or ablation at Samsung Medical Center and had glycemic burden assessment were analyzed. Glycemic burden was assessed using hemoglobin A1c (HbA1c) level. Outcomes were recurrence and overall survival. Risks of recurrence and overall survival were compared according to glycemic burden using a cut-off point of 6.5% or two cut-off points of 6.0% and 7.5%. Overall, 51 (37.2%) patients experienced HCC recurrence. The adjusted hazard ratio (aHR) for recurrence comparing patients with HbA1c > 6.5% to those with HbA1c ≤ 6.5% was 2.66 (95% CI: 1.26-5.78). The risk of recurrence increased in a dose-dependent manner by glycemic burden; aHR for 6.0 < HbA1c ≤ 7.5%: 2.00 (95% CI: 0.78-5.55); aHR for HbA1c > 7.5%: 6.05 (95% CI: 2.31-17.5). Mortality was observed in 16 (11.7%) patients. The risk of mortality was higher for HbA1c > 6.5% than for HbA1c ≤ 6.5% (aHR: 2.33; 95% CI: 1.10-5.08). There was also a dose-response relationship between overall survival and glycemic burden. Glycemic burden assessed using HbA1c level was significantly associated with outcomes of early-stage HCC patients. Good glycemic control could be a therapeutic goal to improve clinical outcomes in these populations.
Keywords: HbA1c; IGF-1; diabetes mellitus; glycemic burden; hepatocellular carcinoma.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Cause-specific risk of major adverse cardiovascular outcomes and hypoglycemic in patients with type 2 diabetes: a multicenter prospective cohort study.Endocrine. 2019 Jan;63(1):44-51. doi: 10.1007/s12020-018-1715-0. Epub 2018 Aug 18. Endocrine. 2019. PMID: 30121774 Clinical Trial.
-
The influence of postoperative glycemic control on recurrence after curative resection in diabetics with hepatitis C virus-related hepatocellular carcinoma.J Surg Oncol. 2012 May;105(6):606-11. doi: 10.1002/jso.22137. Epub 2011 Nov 7. J Surg Oncol. 2012. PMID: 22065536
-
Glycemic burden and the risk of adverse hepatic outcomes in patients with chronic hepatitis B with type 2 diabetes.Hepatology. 2023 Feb 1;77(2):606-618. doi: 10.1002/hep.32716. Epub 2022 Sep 21. Hepatology. 2023. PMID: 36130882
-
Percutaneous ethanol injection or percutaneous acetic acid injection for early hepatocellular carcinoma.Cochrane Database Syst Rev. 2015 Jan 26;1(1):CD006745. doi: 10.1002/14651858.CD006745.pub3. Cochrane Database Syst Rev. 2015. PMID: 25620061 Free PMC article. Review.
-
Management of people with early- or very early-stage hepatocellular carcinoma: an attempted network meta-analysis.Cochrane Database Syst Rev. 2017 Mar 28;3(3):CD011650. doi: 10.1002/14651858.CD011650.pub2. Cochrane Database Syst Rev. 2017. PMID: 28351116 Free PMC article. Review.
References
-
- Omata M., Cheng A.L., Kokudo N., Kudo M., Lee J.M., Jia J., Tateishi R., Han K.H., Chawla Y.K., Shiina S., et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017;11:317–370. doi: 10.1007/s12072-017-9799-9. - DOI - PMC - PubMed
-
- Reig M., Forner A., Rimola J., Ferrer-Fàbrega J., Burrel M., Garcia-Criado Á., Kelley R.K., Galle P.R., Mazzaferro V., Salem R., et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022;76:681–693. doi: 10.1016/j.jhep.2021.11.018. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
