

Coronary Artery Plaque Phenotype and 5-Year Clinical Outcomes in Older Patients with Non-ST Elevation Acute Coronary Syndrome
- PMID: 39076483
- PMCID: PMC11267207
- DOI: 10.31083/j.rcm2505168
Coronary Artery Plaque Phenotype and 5-Year Clinical Outcomes in Older Patients with Non-ST Elevation Acute Coronary Syndrome
Abstract
Background: Lesions with thin-cap fibroatheroma (TCFA), small luminal area and large plaque burden (PB) have been considered at high risk of cardiovascular events. Older patients were not represented in studies which demonstrated correlation between clinical outcome and plaque characteristics. This study aims to investigate the prognostic role of high-risk plaque characteristics and long-term outcome in older patients presenting with non-ST elevation acute coronary syndrome (NSTEACS).
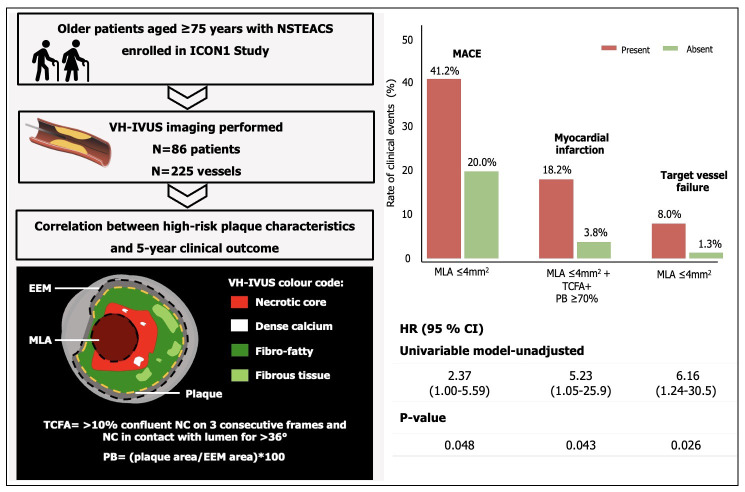
Methods: This study recruited older patients aged 75 years with NSTEACS undergoing virtual-histology intravascular ultrasound (VH-IVUS) imaging from the Improve Clinical Outcomes in high-risk patieNts with acute coronary syndrome (ICON-1). Primary endpoint was the composite of major adverse cardiovascular events (MACE) consisting of all-cause mortality, myocardial infarction (MI), and any revascularisation. Every component of MACE and target vessel failure (TVF) including MI and any revascularisation were considered as secondary endpoints.
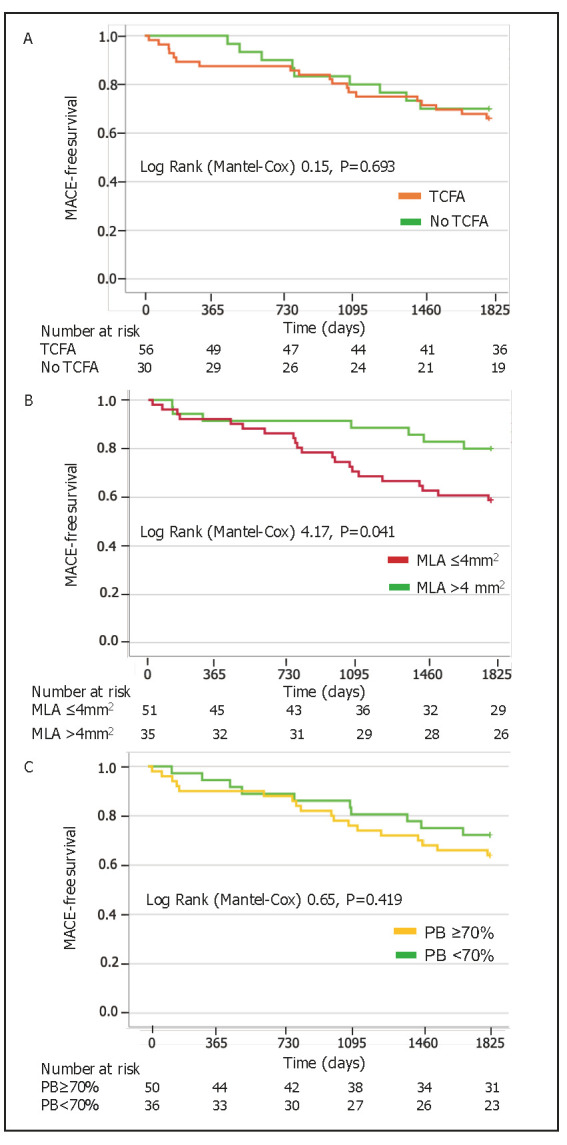
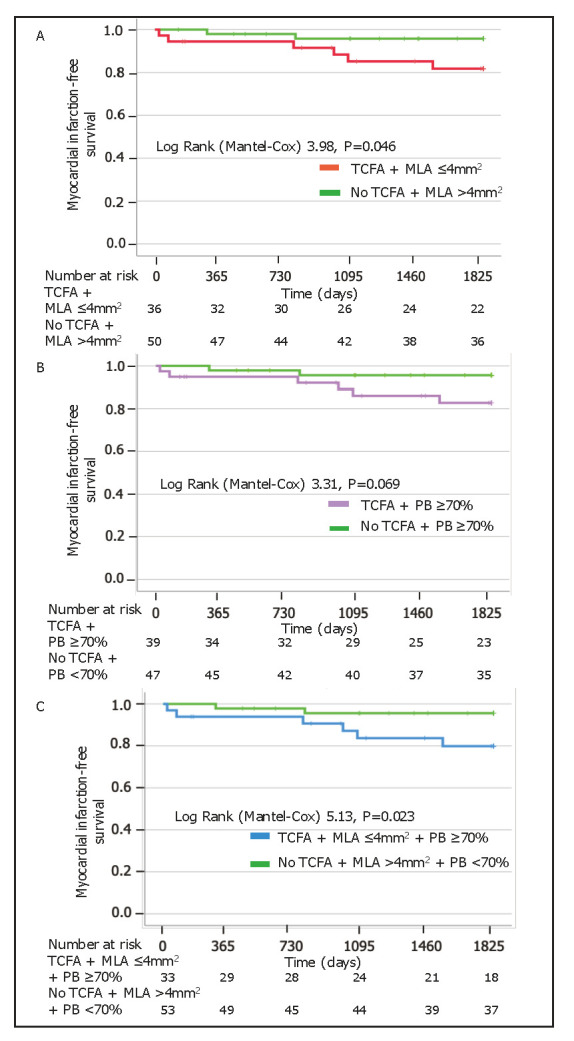
Results: Eighty-six patients with 225 vessels undergoing VH-IVUS at baseline completed 5-year clinical follow-up. Patients with minimal lumen area (MLA) 4 demonstrated increased risk of MACE (hazard ratio [HR] 2.37, 95% confidence interval [CI] 1.00-5.59, p = 0.048) with a worse event-free survival (Log Rank 4.17, p = 0.041) than patients with MLA 4 . Patients with combination of TCFA, MLA 4 and PB 70% showed high risk of MI (HR 5.23, 95% CI 1.05-25.9, p = 0.043). Lesions with MLA 4 had 6-fold risk of TVF (HR 6.16, 95% CI 1.24-30.5, p = 0.026).
Conclusions: Small luminal area appears as the major prognostic factor in older patients with NSTEACS at long-term follow-up. Combination of TCFA, MLA 4 and PB 70% was associated with high risk of MI.
Clinical trial registration: NCT01933581.
Keywords: major adverse cardiovascular events; minimal lumen area; non-ST elevation acute coronary syndrome; older patients; plaque burden; thin-cap fibroatheroma; virtual-histology intravascular ultrasound.
Copyright: © 2024 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Non-fibroatheroma lesion phenotype and long-term clinical outcomes: a substudy analysis from the PROSPECT study.JACC Cardiovasc Imaging. 2013 Aug;6(8):908-16. doi: 10.1016/j.jcmg.2013.04.008. Epub 2013 Jul 10. JACC Cardiovasc Imaging. 2013. PMID: 23850249
-
Coronary artery lesion phenotype in frail older patients with non-ST-elevation acute coronary syndrome undergoing invasive care.EuroIntervention. 2019 Jun 12;15(3):e261-e268. doi: 10.4244/EIJ-D-18-00848. EuroIntervention. 2019. PMID: 30777840
-
Impact of positive and negative lesion site remodeling on clinical outcomes: insights from PROSPECT.JACC Cardiovasc Imaging. 2014 Jan;7(1):70-8. doi: 10.1016/j.jcmg.2013.10.007. JACC Cardiovasc Imaging. 2014. PMID: 24433710 Clinical Trial.
-
In vivo detection of high-risk coronary plaques by radiofrequency intravascular ultrasound and cardiovascular outcome: results of the ATHEROREMO-IVUS study.Eur Heart J. 2014 Mar;35(10):639-47. doi: 10.1093/eurheartj/eht484. Epub 2013 Nov 19. Eur Heart J. 2014. PMID: 24255128 Clinical Trial.
-
Adiponectin in Relation to Coronary Plaque Characteristics on Radiofrequency Intravascular Ultrasound and Cardiovascular Outcome.Arq Bras Cardiol. 2018 Sep;111(3):345-353. doi: 10.5935/abc.20180172. Arq Bras Cardiol. 2018. PMID: 30379252 Free PMC article.
References
-
- Vaduganathan M, Mensah GA, Turco JV, Fuster V, Roth GA. The Global Burden of Cardiovascular Diseases and Risk: A Compass for Future Health. Journal of the American College of Cardiology . 2022;80:2361–2371. - PubMed
-
- Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, et al. Heart Disease and Stroke Statistics-2022 Update: A Report from the American Heart Association. Circulation . 2022;145:e153–e639. - PubMed
-
- Naghavi M, Libby P, Falk E, Casscells SW, Litovsky S, Rumberger J, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part I. Circulation . 2003;108:1664–1672. - PubMed
-
- Virmani R, Burke AP, Farb A, Kolodgie FD. Pathology of the vulnerable plaque. Journal of the American College of Cardiology . 2006;47:C13–C18. - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
