

Predicting the occurrence of minor adverse events in cardiac rehabilitation using physical variables
- PMID: 39060357
- PMCID: PMC11282225
- DOI: 10.1038/s41598-024-68223-y
Predicting the occurrence of minor adverse events in cardiac rehabilitation using physical variables
Abstract
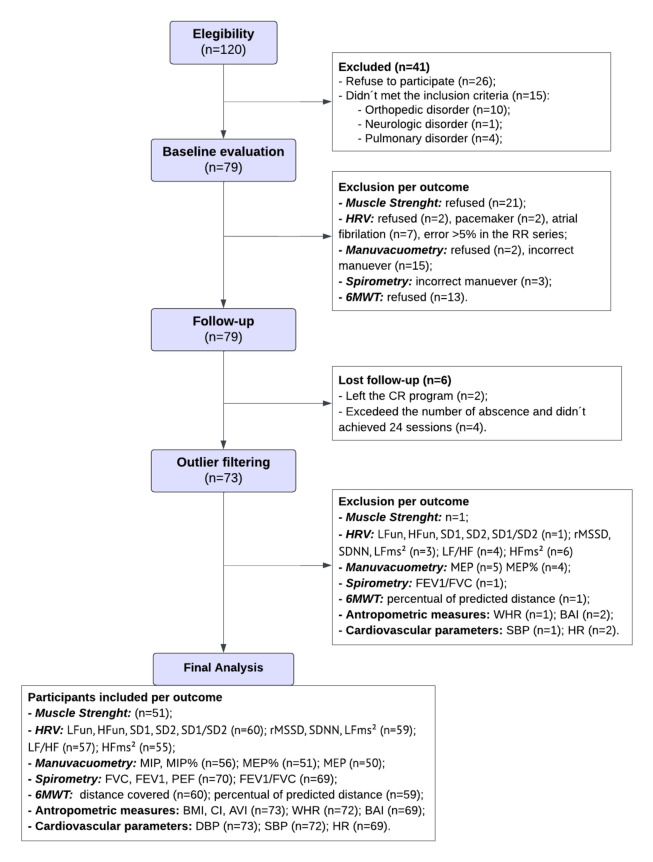
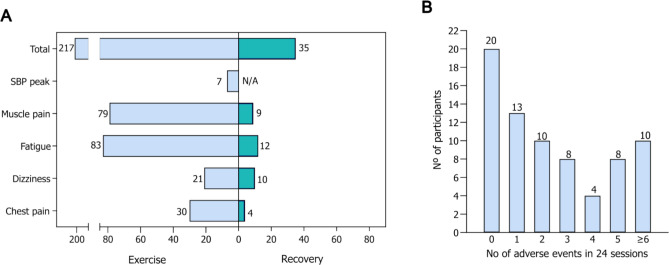
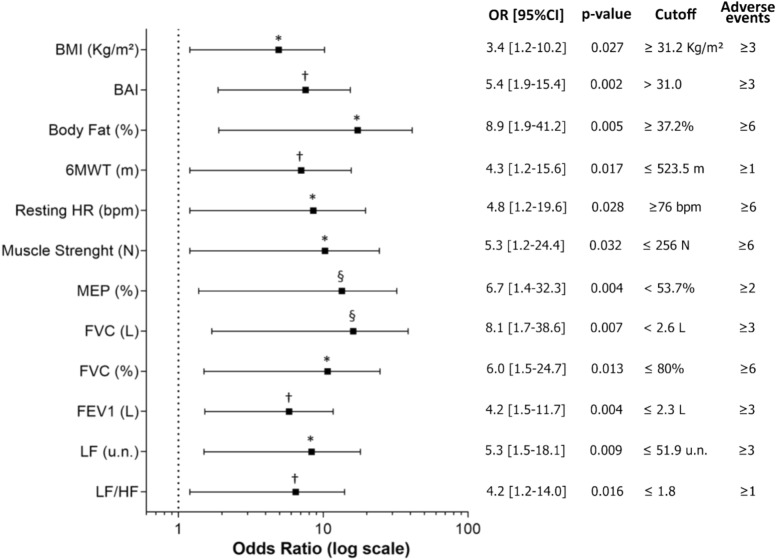
The safety of exercise practice by individuals with cardiovascular disease is due to a good clinical evaluation to identify patients with a higher risk of adverse events, thus the study of simple variables capable of predicting the rate of events during exercise is relevant and may provide better screening tools to be applied in the clinical practice. The study aimed to evaluate if clinical and physical parameters can predict the rate of adverse events during exercise-based cardiac rehabilitation. This was a cohort study that followed 73 patients during 24 sessions of exercise. Were registered 217 simple adverse events, at a rate of 2.5 events per hour of exercise. We found that higher adiposity, worse pulmonary function, lower functional capacity, and reduced heart rate variability were significant and acceptable predictors of adverse events during exercise, according to the ROC curve analysis. We state that these simple physical parameters may be useful for cardiac risk stratification in cardiac rehabilitation programs with low resources, contributing to its safety.
Keywords: Acute events; Cardiac rehabilitation; Cardiovascular diseases; Exercise; Risk factors.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Exercise training-induced modification in autonomic nervous system: An update for cardiac patients.Ann Phys Rehabil Med. 2017 Jan;60(1):27-35. doi: 10.1016/j.rehab.2016.07.002. Epub 2016 Aug 16. Ann Phys Rehabil Med. 2017. PMID: 27542313 Review.
-
Efficacy and safety of exercise rehabilitation in patients with hypertrophic cardiomyopathy.J Cardiol. 2019 Nov;74(5):466-472. doi: 10.1016/j.jjcc.2019.04.013. Epub 2019 Jun 22. J Cardiol. 2019. PMID: 31235420
-
Effectiveness of Intensive Cardiac Rehabilitation in High-Risk Patients with Cardiovascular Disease in Real-World Practice.Nutrients. 2021 Oct 29;13(11):3883. doi: 10.3390/nu13113883. Nutrients. 2021. PMID: 34836144 Free PMC article.
-
Exercise and cardiovascular events: Is there any J curve relation?Hellenic J Cardiol. 2017 Sep-Oct;58(5):391-392. doi: 10.1016/j.hjc.2017.11.015. Epub 2017 Dec 9. Hellenic J Cardiol. 2017. PMID: 29233737 No abstract available.
-
Safety of home-based cardiac rehabilitation: A systematic review.Heart Lung. 2022 Sep-Oct;55:117-126. doi: 10.1016/j.hrtlng.2022.04.016. Epub 2022 May 6. Heart Lung. 2022. PMID: 35533492 Review.
References
-
- American Association of Cardiovascular & Pulmonary Rehabilitation. Guidelines for Cardiac Rehabilitation Programs. (Human Kinetics, Champaing, 2021).
-
- Thompson, P. D. et al. Exercise and acute cardiovascular events placing the risks into perspective: A scientific statement from the American heart association council on nutrition, physical activity, and metabolism and the council on clinical cardiology. Circulation115, 2358–2368 (2020). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
